


 According to Dr. Chilkov, “keto” has advantages and downsides. “You have to manage these patients very, very carefully. Cancer patients should not try to do keto regimens on their own.” Done properly, ketogenic diets impede tumor growth, reduce angiogenesis, quell inflammation, and increase apoptosis. But strict keto or “paleo” diets tend to make cancer patients nauseous, and often induce diarrhea, owing to their very high fat content.
According to Dr. Chilkov, “keto” has advantages and downsides. “You have to manage these patients very, very carefully. Cancer patients should not try to do keto regimens on their own.” Done properly, ketogenic diets impede tumor growth, reduce angiogenesis, quell inflammation, and increase apoptosis. But strict keto or “paleo” diets tend to make cancer patients nauseous, and often induce diarrhea, owing to their very high fat content.
Most of the popular keto protocols call for 60-85% of total calories from fat, with 10-30% as protein, and only 2-10% carbohydrates. Cancer patients who do try ketogenic or paleo protocols will likely need pancreatic enzymes, and/or ox bile, to aid in fat digestion.
“Strict keto is not a healthy long-term diet for cancer patients. It is a therapeutic diet to achieve a particular goal.” Long periods on keto or paleo diets can lead to significant microbiome changes, and not always for the good. People on these diets long-term often show weird variances in the ratios between different microbial species, as well as . higher susceptibility to leaky gut.
The reality is, it is difficult for most people to stay with strict keto over the long term.
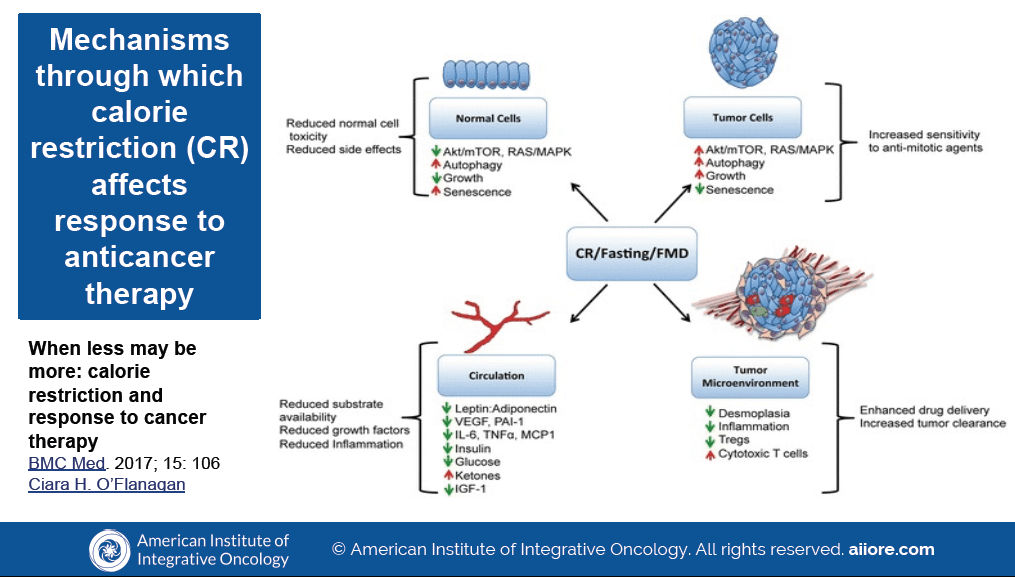
“You can get a lot of benefits with a modified keto diet: low glycemic, carb-restricted, with moderate protein can give a lot of the benefits in terms of changing the tumor microenvironment, without a lot of the downsides of the strict keto approach.
If you reduce carbs to 10-20% of total dietary intake, you do slow tumor growth,” Dr. Chilkov says, citing a 2011 paper by Ho and colleagues at the University of British Columbia.
The OutSmart Cancer Diet
“The main thing is, you need diets that people can stay on.”
With that in mind, she developed a basic diet protocol she calls the Outsmart Cancer diet. It is a mostly plant-based, moderate-protein, low-carb whole foods diet that stresses the following:
Limited dairy and animal-derived proteins and fats; Reduced glycemic load; Increased intake of colorful phytonutrients, cruciferous vegetables, and sulfur-containing foods (garlic, onions); Daily consumption of fermented vegetables; Liberal use of monounsaturated fats and oils; Increased spices and herbs, High fluid intake; Elimination of pro-inflammatory foods; Limited alcohol intake, and as much organic unprocessed unrefined food as possible.
On this diet, roughly 25-40% of total intake is protein, with 30-45% being fat, and 10-25% as carbs. It is higher in protein and lower in fat than most ketogenic diets.
“I go for around 60g protein per day. If a patient is sarcopenic, however, he or she will need more. Preferably vegan protein. Too much animal protein drives cancer growth.”
Do all cancer patients need to go full-on vegan? Not necessarily.
There’s ample evidence that plant-based diets benefit cancer survivors. Chilkov says she does recommend vegetarian and vegan diets, but doesn’t push them. 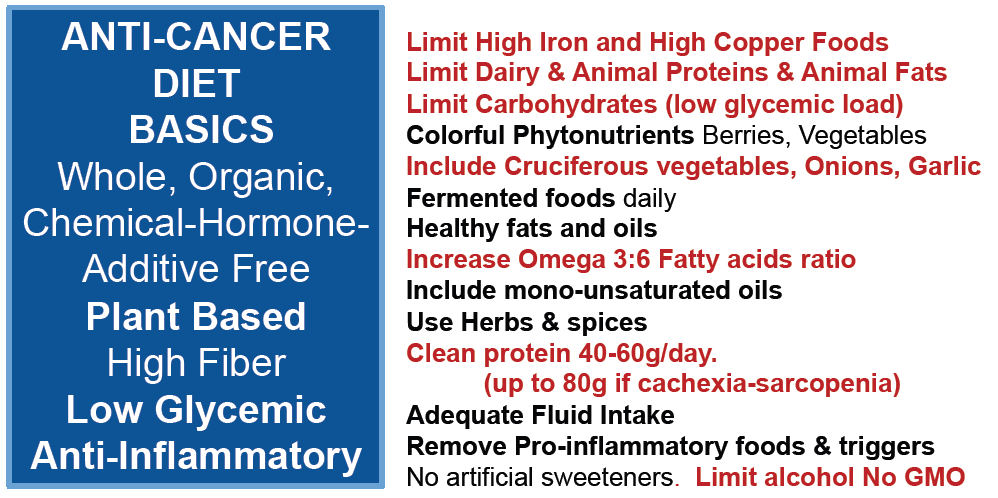 The main thing is to encourage patients to eat as many vegetables and fruits as they can.
The main thing is to encourage patients to eat as many vegetables and fruits as they can.
“Once you get up to 40-50% of someone’s daily intake as plant-based foods, you start to see reduced occurrence and recurrence of cancer.”
Be aware that patients who do go vegetarian or vegan will likely need to supplement with Omega-3s and B vitamins. Also keep in mind that vegetarian diets can be very high-glycemic. “These patients need to be on low-carb vegetable-based diets”
She likes to see all her patients getting a lot of fiber—ideally in the range of 25-35 g/d. Most Americans typically get only 15. The caveat is that some cancer patients may be at risk for bowel obstructions. In these cases, it is wise to limit fiber.
Cancer patients should be careful to limit iron and copper intake. If someone has true iron deficiency anemia, he or she will need repletion. But for many cancer patients, excessive iron and copper can be detrimental. Both minerals may play a role in promoting cancer. This means not too much in the way of nuts and seeds.
Dr. Chilkov’s OutSmart Cancer diet generally eliminates lard, which is advocated by some keto/paleo enthusiasts. She prefers olive oil, avocado oil, or grass-fed butter.
Though her recommendations are largely veg-based, Dr. Chilkov is a big fan of bone broth, especially for patients who have mucositis, gastritis, nausea or reduced appetite. “Bone broth is very nutritious, contains lots of collagen, minerals, and electrolytes. For some patients, 4-6 cups per day is great.” The caveat is that it needs to be made from high quality organic, and ideally grass-fed, meats.
That’s because environmental toxins concentrate in fat and bone. Cancer patients definitely do not need any further toxic strains.
Eggs are another animal-derived food that some patients may want to include. “So long as a patient does not have any allergies to eggs or sensitivities to albumin, and not a vegan, eggs are an excellent source of protein. If patients do want to eat them, she advises them to seek high quality, high omega-3 fortified eggs.
Fasting & Fast-Mimicking Diets
This approach is getting a lot of media attention these days, thanks to the work of Valter Longo, PhD, the University of Southern California-Davis cell biologist/gerontologist who is one of the most outspoken scientific advocates for fasting. Longo’s popular book, The Longevity Diet, his TED talks, and his widely publicized early-stage clinical trials, have amplified the notion of fast-mimicking in the media.
According to Dr. Chilkov, Longo’s recommendations make for a very sound cancer-fighting, health promoting diet. However, she acknowledged that beyond anecdote, clinical experience, and some very early clinical data, there is little definitive human research on these approaches. So they’re not yet truly “evidence-based.”
Cancer patients who do want to try intermittent fasting need to be careful. “If they’re relatively young and relatively healthy, they can safely fast for 48 hours. But patients who are fragile shouldn’t fast at all.” She added that, “my feeling is that cancer patients need a lot of nourishment.”
Raw Food Diets
Though raw food diets are promoted as “healthy” and “cancer fighting,” for their high phytonutrient and fiber content, many cancer patients cannot handle a lot of raw vegetables, nuts, and fruits. While it is good to include some, the approach should not be extreme. She advises cancer patients not to eat raw meat and fish, because they increase exposure to bacteria and molds. That may not be problematic for healthy people, but it can be for cancer patients with compromised immune systems.
Also, be aware that some phytochemicals—lycopene in tomatoes, sulforaphane in broccoli, for example—are only released when the vegetables are lightly cooked. They are liberated by heat. This is one reason why steaming is a preferred method for cooking vegetables.
Soy
“Soy is so controversial and so misunderstood,” said Dr. Chilkov. Yes, it is a source of isoflavones which are plant estrogens. But traditional fermented soy products are seldom problematic and often beneficial for people with cancer.
A 2008 analysis of 8 separate studies showed that women with the highest soy intake (including soy milk, tofu, and similar soy foods) had a 29% lower lifetime risk of breast cancer compared with women who did not eat soy. A 2014 review of 35 studies put that risk reduction at 41%. And a 2012 analysis of over 9,500 breast cancer survivors showed a 30% reduction in recurrence among the women who ate the most soy.
It is true that some people do not tolerate soy very well, but most will benefit from fermented soy foods. And there’s little risk if they are eating traditional fermented soy foods (miso, tofu, tempeh, natto).
The problems come with modern unfermented soy products and isolates. She strongly advises against products made from genetically-modified soy—which, unfortunately, means many of the mainstream mass-market soy products.
Citing a comprehensive 2013 review paper by Don Abrams and Mary Hardy, Dr. Chilkov insisted that it is high time for clinicians to reconsider their biases against soy.
Gluten
Some thought leaders within the functional medicine world contend that there is a direct link between gluten and cancer, but this is very far from solidly evidence-based, said Dr. Chilkov. That said, gluten can trigger systemic inflammation in some patients, and that is cancer-promoting. So, it is probably a good idea for cancer patients to eliminate—or at least minimize–their gluten intake.
Her Outsmart Cancer diet is largely gluten-free. “Eliminate the refined carbs, and you will eliminate a lot of the gluten.” But she only pushes a strict gluten-free diet if a patient has brain fog, depression and signs of autoimmune disease, and/or colorectal cancer.
Hydration & Shakes
Hydration is vital, especially for cancer patients during chemotherapy. Plain water is a must, and vegetable broths and/or bone broths are also very nourishing and hydrating.
The reality is, many cancer patients have limited appetites or, owing to myositis and mucositis, they experience a lot of pain when trying to eat solid food.
For them, protein rich shakes and smoothies are ideal. She recommends a ketogenic shake recipe containing 30-40 grams of whey or collagen protein (pea or rice protein for vegetarians), medium chain fatty acids, concentrated red and green powders, pumpkin seeds, a whole lemon and a host of other ingredients (see sidebar).
“One or two of these shakes can get cancer patients through a full day, if they’re having difficulty eating solid food,” she said.
Exercise
If a patient has the strength to exercise, encourage participation in whatever forms of reasonable non-strenuous activity he or she enjoys. The benefits are many. She noted that she regularly collaborates with an oncologist who has patients running on treadmills while getting their chemotherapy infusions. “They’re not necessarily invalids,” she stressed.
Practical Implementation
Dr. Chilkov is the first to admit that it can be very challenging to do nutritional counseling for cancer care in a medical context. First, it requires a fair amount of knowledge. To this end she has compiled an intensive online clinician training course called Foundations of Integrative Oncology.
It also takes a fair amount of counseling skill and patience. Lifestyle changes are never easy, even with very motivated patients. Physicians are not always ideally trained to do this sort of work. Nutritionists and health coaches are.
In her practice, she has two nutritionists that work directly with the patients to help make the recommended lifestyle shifts.
To do this work well, it is equally important to develop strong collegial relationships with oncologists in your area. That means recognizing the limitations of natural medicine, and the value of conventional modalities. You want to work with each patient’s oncology team, and avoid adversarial stances. The worst thing you can do is put a patient in the middle of a contention between yourself and her specialists.
“I’m not anti- standard of care, and I’m careful not to interfere with the oncologists,” she said. “I’m a consummate ‘middle of the road’ practitioner. I don’t do a lot of really radical things.”
Conventional oncologists and cancer treatment centers vary widely in their stances on supplements, diet therapies, and other “alternative” strategies. Some centers, like Memorial Sloan Kettering and City of Hope have strict institutional policies against patients using herbs and supplements while undergoing treatment there. At others, like Cancer Treatment Centers of America, nutraceuticals, herbs and a host of naturopathic therapies are an integral part of the care protocols.
The important thing is cultivating mutual respect with conventional medical colleagues. “What I say to oncologists is, ‘You be the disease expert. Let me become the health expert. Many of my patient referrals actually come from the oncologists.”
END


