



A small but compelling case series published last year suggests that mega-doses of vitamin D can yield dramatic improvement in the severity of longstanding psoriasis. And by “mega,” we mean doses as high as 60,000 IU per day.
Renu Mahtani, a physician at the Autoimmunity Treatment Centre, Pune, India, together with Pradeep M.K. Nair of the Sant Hirdaram Medical College of Naturopathy in Bhopal, treated six patients—five women and one man—with high-dose oral vitamin D (25-hydroxy cholecalciferol) for periods of 2-6 months, in the absence of other concomitant psoriasis therapies.
The patients ranged in age from 48 to 63 years, and all had moderate to severe psoriasis for between 2-30 years. Three had psoriasis vulgaris, and the others had the palmoplantar form of the disease.
Prior to treatment, the physicians measured each patient’s baseline serum vitamin D levels. Four were within normal range, and they began treatment with 30,000 IU of oral D3 per day. Two showed severe deficiencies, and began with a one-time loading dose of 60,000 IU per day, then continued with 30,000 IU per day like the others.
Every other month, Drs. Mahtani and Nair measured parathyroid hormone (PTH) levels. PTH is inversely correlated with serum vitamin D; typically, it is high when vitamin D is low, and it drops when vitamin D levels rise.
People with psoriasis and other autoimmune disorders sometimes have genetic polymorphisms of the vitamin D receptors which blunt the tissue effects of the vitamin. In other words, they are functionally deficient, though their serum levels of the vitamin may be normal.
They used PTH changes, along with observations of clinical response, as a guide in adjusting each patient’s vitamin D dose upward or downward. However, they cautioned that, “due to the Vitamin D resistance…found in those with autoimmune disorders, the drop in PTH could be suboptimal, warranting an increase in the dose of vitamin D to combat this resistance.”
Drs. Mahtani and Nair also measured ionized calcium levels, as a safeguard against hypercalcemia which sometimes occurs following prolonged high-dose vitamin D supplementation.
Obvious Benefits
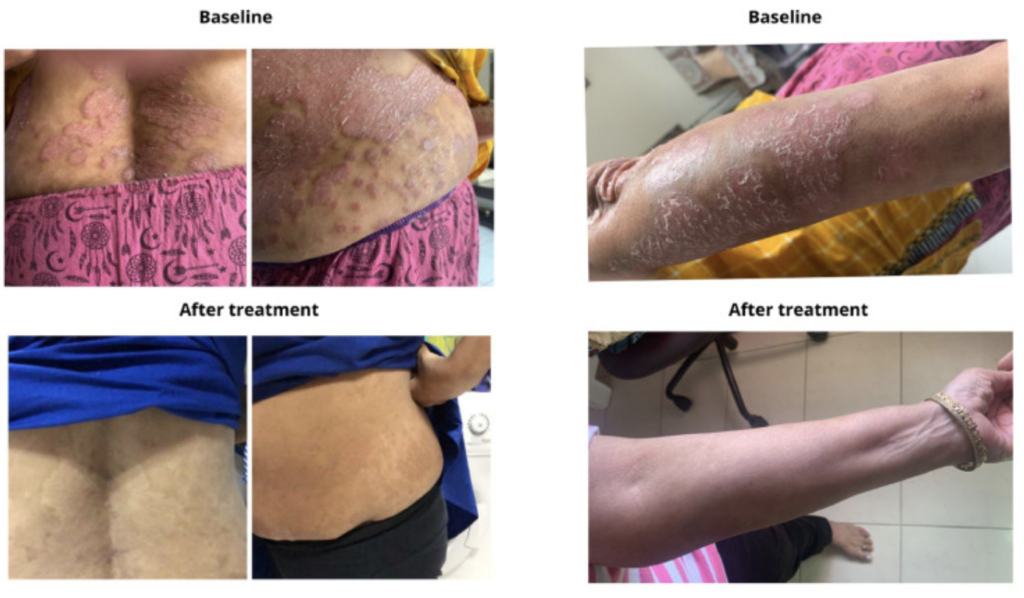
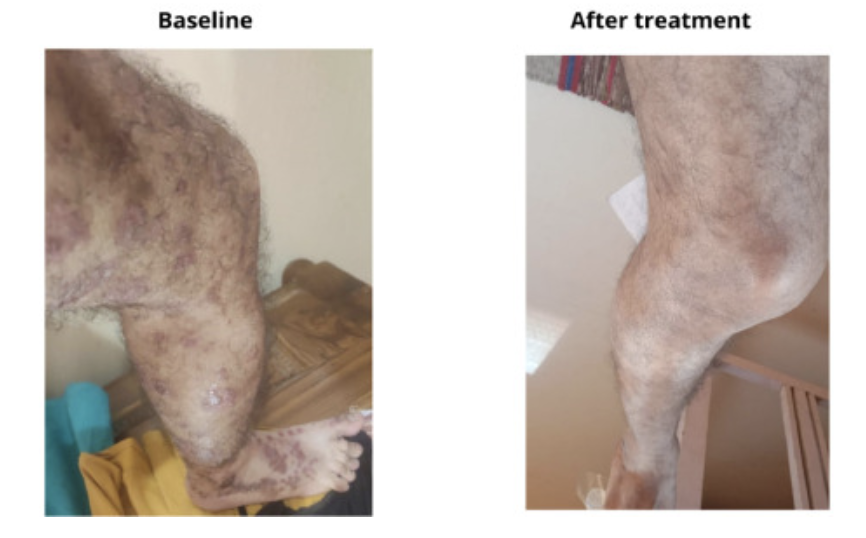
The therapeutic impact of vitamin D was quite impressive, and readily visible even to an untrained eye.
All six patients showed marked reductions in lesion number, thickness, and severity within 3-6 months of supplementation. The improvements correlated with major reductions in the patients’ PASI (Psoriasis Area and Severity Index) scores.
The paper describes each case in detail.

“Observations from this case series demonstrate promising and durable control of the signs and symptoms in psoriasis, with no adverse events or relapse after regular oral supplementation of Vitamin D3,” wrote Mahtani and Nair (Mahtani R, Nair PMK. Clin Immunol Comm. 2022).
They added that adherence to the supplement protocols approached 100%, “as the patients were motivated by the results.
“Observations from this case series demonstrate promising and durable control of the signs and symptoms in psoriasis, with no adverse events or relapse after regular oral supplementation of Vitamin D3.”
–Renu Mahtani & Pradeep M.K. Nair
A Key Pathogenic Factor
In their report, the authors state that many previous researchers have reported inverse relationships between serum D3 levels and the severity and progression of psoriasis and other autoimmune disorders.
The vitamin plays an important role in regulating keratinocytes—the key cells involved in the pathology of psoriasis. This relationship is also inverse: low circulating vitamin D levels promote keratinocyte proliferation—the hallmark of psoriasis—while high blood levels inhibit proliferation (Barrea L, et al. Rev Endocr Metab Disorders. 2017, Reichrath J. Exper Dermatol. 2007).
The regulatory effects of D3 on keratinocytes were initially described by researchers at Osaka University School of Medicine back in 1990, based on a series of cell culture experiments. Since then, several human studies have suggested a strong link between vitamin D deficiency and psoriasis.
In 2012, dermatologist Paolo Gisondi and colleagues at the University of Verona, Italy, published a year-long, cross-sectional study comparing vitamin D levels in145 people with chronic plaque psoriasis, 112 with rheumatoid arthritis (RA), and 141 heathy control subjects.
They found that the prevalence of deficiency, while high across the board, was highest among the people with psoriasis—58%, versus 38% among those with RA, and 30% in the control group. During the winter season, deficiency rates reached a staggering 81% in the psoriasis group (Gisondi P, et al. Br J Dermatol. 2012).
Low circulating vitamin D levels promote keratinocyte proliferation—the hallmark of psoriasis—while high blood levels inhibit proliferation.
Dermatologists at San Cecilio University Hospital, Grenada, Spain, showed that a cohort of 46 people with psoriasis had markedly lower serum 25-OHD levels compared with a matched cohort of healthy control subjects. The mean values were 30.5 versus 38.3 ng/ml, a statistically significant difference (Orgaz-Molina J, et al. Acta Derm Venereol. 2014).
Vitamin D Resistance
But 4 of the 6 patients in the Mahtani-Nair cohort had baseline vitamin D levels within normal range. This underscores an important point: people with psoriasis and other autoimmune disorders sometimes have genetic polymorphisms of the vitamin D receptors which blunt the tissue effects of the vitamin (Zhang F, et al. Curr Cardiovasc Risk Reports. 2012; Finamor DC, et al. Dermatoendocrinol. 2013).
In other words, these people are functionally deficient, though their serum levels of the vitamin may be normal, and they will likely need markedly higher supplementation doses to obtain the desired effects.
In their 2021 review paper, Lemke and colleagues go as far as stating that genetically-predisposed or acquired vitamin D resistance is a primary pathologic mechanism for most if not all autoimmune disorders, including psoriasis (Lemke D, et al. Front Immunol. 2021).
Topical calcipotriol and other prescription vitamin D3 analogs have been mainstay treatments for psoriasis for many years. A 2009 Cochrane Systematic Review of 131 studies concluded that topical D3 analogs are definitely more effective than placebo ointments, and comparable to the more powerful but side-effect ridden topical steroids (Mason A, et al. Cochrane Database Syst Rev. 2009).
A First Line Therapy?
Yet, despite the apparent connection between systemic vitamin D deficiency and the etiology of psoriasis, researchers have never seriously explored the possibility that vitamin D supplementation could be preventive or therapeutic. Mahtani and Nair contend that theirs is the first case series documenting the safety and efficacy of high-dose oral supplementation as a treatment for psoriasis.
While acknowledging that their case series is not a definitive clinical trial, they hold that it is time for researchers and clinicians alike to take vitamin D supplementation seriously as a first-line modality for people with psoriasis.
“Optimal doses of Vitamin D enhances both the natural and adaptive immunity, which makes this practice effective and worth considering over the present day management of psoriasis with immunosuppressive drugs,” they write.
Mechanistically, there’s a strong case to support vitamin D in the management of psoriasis. The condition is characterized by excessive keratinocyte proliferation and dysregulated immune activity. Vitamin D appears to modulate both.
Multiple Mechanisms
Deficiency, whether frank or functional, can lead to unchecked immune activity, contributing to the inflammation and immune responses typical of psoriasis. The vitamin influences the balance between regulatory T cells and pro-inflammatory cytokines, which in part determines the severity of psoriatic lesions.
It is time for researchers and clinicians alike to take vitamin D supplementation seriously as a first-line modality for people with psoriasis.
Mahtani and Nair attribute the dramatic effects they saw, in part, to the effect of the vitamin on monocytes, macrophages, T cells, and dendritic cells, all of which play important roles in the etiology of psoriasis.
Vitamin D and its receptors also influence the integrity of intracellular tight junctions, which has major implications for barrier function of the skin, and also potentially, of the gut epithelium.
Visconti and colleagues at the Sapienza University of Rome showed that the number of vitamin D receptors was markedly lower in skin tissue samples from 20 people with psoriasis, compared with samples from normal non-psoriatic individuals. This correlated with differences in expression of tight junction proteins (Visconti B, et al. Dermatol & Venereol. 2015).
Safe at High Levels
In terms of safety, Mahtani and Nair state that they saw no adverse effects associated with high-dose oral vitamin D. In 5 of the 6 reported cases, the patients were able to reduce their daily doses down from 30,000 IU to 20,000 or even 10,000, after several weeks.
Only one patient needed a dose increase, from 30,000 IU up to 60,000 for several months, after which she was able to cut down, in 10,000 IU increments, to a maintenance dose of 40,000 IU. In this case, the physicians advised the patient to strictly limit her intake of calcium-rich foods, to avert the possibility of hypercalcemia.
All six patients remained recurrence-free, while on maintenance doses of 10,000-40,000 per day. This begs the question of what would happen if they were to stop their supplementation. It’s an important consideration, and one that ought to be addressed in future clinical trials looking at the impact of vitamin D in psoriasis.
END


