




Fish oil is a commonly recommended holistic treatment for joint pain. Does krill oil — a related supplement with strong anti-inflammatory properties — impart similar benefits?
The answer is “Yes,” according to researchers at the Commonwealth Scientific and Industrial Research Organisation (CSIRO), Australia’s national science agency.
A large CSIRO study of a commercially available krill oil supplement showed that patients with knee osteoarthritis (OA) obtained modest but meaningful improvements in knee pain, stiffness, and physical function after supplementing with krill oil.
The investigators concluded that krill oil was safe, and presents an effective alternative to conventional OA treatments. The study was published in July in The American Journal of Clinical Nutrition (Stonehouse, W et al. Am J Clin Nut. 2022; 116(3): 672–685).
Krill or Fish?
Krill (Euphausia superba) — a diverse group of small marine crustaceans — are among the world’s most abundant species in terms of total biomass. Researchers estimate there are 300,000 million metric tons in the Antarctic Ocean alone.
Like fish, krill are rich in the inflammation-reducing eicosapentaenoic and docosahexaenoic acids (EPA and DHA).
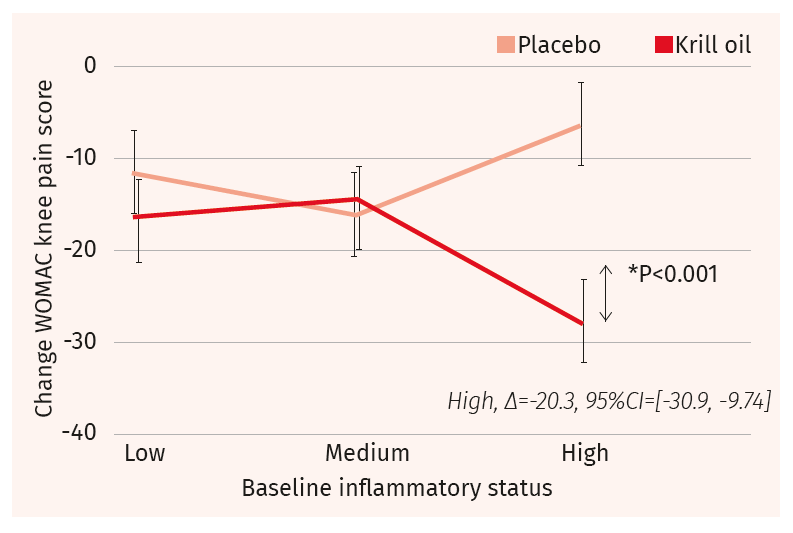
Patients with the highest levels of inflammation at baseline—as indicated by elevated baseline C-reactive protein (hsCRP) levels–experienced significantly greater improvements in knee pain following krill oil treatment than those with low or medium degrees of inflammation at baseline.
Omega-3 supplements generally, and fish oils in particular, are known for their anti-inflammatory effects. Numerous fish oil studies offer evidence of its ability to quell inflammation. The literature on krill oil, however, is far less robust.
The CSIRO team, headed by Dr. Welma Stonehouse, proposed that krill oil could impact OA-related pain via similar anti-inflammatory mechanisms observed for fish oil.

Their randomized, placebo-controlled trial took place at four clinical sites across Australia over six months. It included 235 healthy adults between 40 and 65 years of age. All participants had clinical diagnoses of mild to moderate knee OA and habitually consumed low amounts of long-chain (LC) omega-3 (ω-3) fatty acids in their diets. None used fish oil supplements.
The investigators split the participants into two groups: a treatment group receiving 4 grams of krill oil per day (4 one-gram capsules), and a control group that took a vegetable oil placebo. Participants were instructed to take the assigned capsules with or immediately after a meal.
The krill supplement–a popular Australian retail brand containing the Superba™ BOOST manufactured by Aker BioMarine–provided 1 g krill oil (E. superba oil; 0.15 g EPA, 0.07 g DHA) and 0.11 mg of astaxanthin per capsule, totaling 880 mg of ω-3 and 45 mg astaxanthin daily.
According to the investigators, the recognized dosage at which EPA in combination with DHA typically exert an anti-inflammatory response is >2 g per day.
They point out that 73% of the EPA and DHA in Superba krill oil is phospholipid-bound, which they suggest would “facilitate more efficient incorporation of long-chain ω-3 PUFAs into tissues than triglyceride form.” Owing to the fact that the ω-3s are phospholipid-bound, “krill oil’s anti-inflammatory effect would be greater than what would be expected based on its long-chain ω-3 PUFA content alone.”
The 4-gram daily dosage was deliberately set higher than the levels used in prior knee OA studies, “so as to facilitate an anti-inflammatory response, but in amounts suitable as a complementary medicine.”
Supplementation with krill oil translated clearly into an increase in blood ω-3s levels, as indicated by changes in the OmegaQuant Omega-3 Index—a measure of ω-3 content in red blood cell membranes.
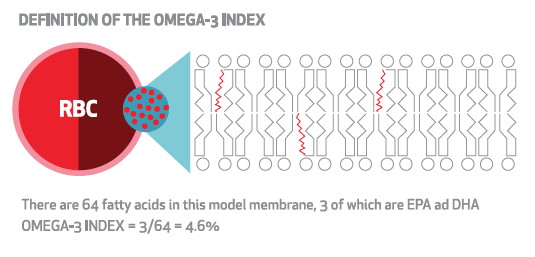
In the krill group, participants’ mean Omega-3 Index increased from 6.0% at baseline to 8.9% at 3 months and to 9.0% at 6 months. In the placebo group, on the other hand, the levels did not change, with Omega-3 Index measurements remaining between 5.4% and 5.5% throughout the study.
Reduced Pain & Stiffness
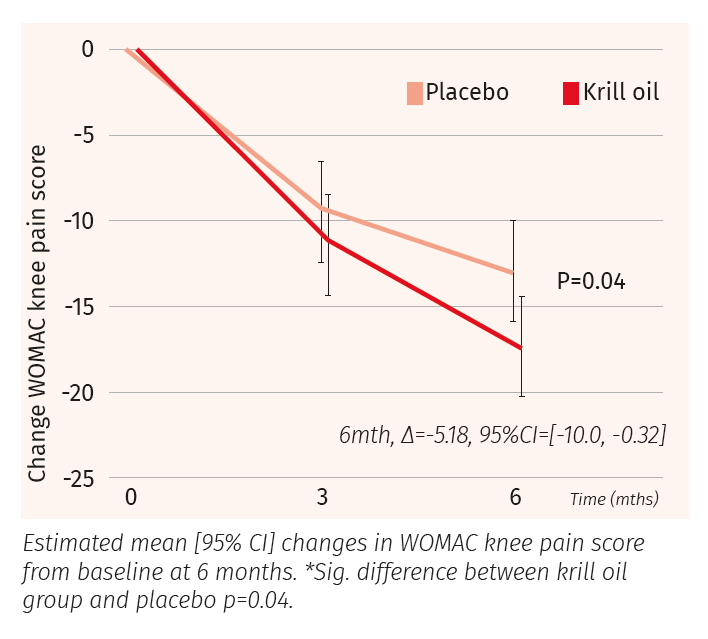
The CSIRO researchers assessed OA severity at baseline, three months, and six months, using a visual analog self-assessment scale. They quantified changes in knee pain, stiffness, and physical function using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scales.
The krill and the placebo groups both showed some degree of improvement of knee pain over the course of the trial, but, the krill group showed a greater decrease. The difference in adjusted mean change between groups at 6 months was −5.18 (95% CI: −10.0, −0.32; P = 0.04).
Closer analysis indicated that patients with the highest levels of inflammation at baseline—as indicated by elevated baseline C-reactive protein (hsCRP) levels–experienced significantly greater improvements in knee pain following krill oil treatment than those with low or medium degrees of inflammation at baseline.
Compared with the placebo group, the patients taking krill oil also showed greater improvements in knee stiffness and physical function. The difference in adjusted mean change of WOMAC scores between the two groups at 6 months was −6.45 for knee stiffness; −4.67 for physical function; and -4.83 for total knee score. All of these changes were statistically significant.
There were no significant differences between the two groups in terms of need for NSAIDs.
Safer Therapies Needed
Though krill oil cannot be considered a “cure” for OA, the results of the Stonehouse study do hold promise for patients who suffer from OA-associated joint inflammation and pain. OA is a major cause of chronic pain and disability worldwide. While conventional drug therapies—typically NSAIDs–may provide some symptomatic relief, they do little to quell the underlying drivers of inflammation.
Stonehouse and colleagues note that, “Owing to the adverse effects associated with long-term NSAID use, there is a need to identify alternative therapies that can safely and effectively reduce pain and inflammation and improve function.”
Krill oil differs structurally from other dietary sources of ω-3 in that it delivers a relatively high amount of ω-3 PUFAs in phospholipid form rather than triglyceride form (the primary source of EPA and DHA in fish oil).
Preliminary research suggests that the ω-3s in krill oil might have a higher bioavailability than those in fish oil. There’s some evidence that krill’s higher relative phospholipid content could facilitate ω-3 incorporation into the tissues more efficiently than fish oil.
Krill also confers the additional inflammation-lowering benefits of astaxanthin, a naturally occurring red pigment that acts as an antioxidant. Astaxanthin exists in only a handful of natural sources, including salmon, shrimp, trout, crayfish, algae, and yeast.
Closing the Research Gap
The CSIRO trial is the largest, longest, and highest-dose krill oil study to date, at least in the context of OA. The main result was a significant increase in Omega-3 Index to 9% after 6 months, which translated into a modest but significant reduction in knee pain and stiffness, and improvements in physical function of affected joints.
Prior to the CSIRO trial, studies of krill supplementation and OA were mostly small, short, and used very low krill dosages.
In addition to confirming krill oil’s anti-inflammatory properties, the CSIRO data showed that it is remarkably safe. There were no worrisome adverse events during the 6-month trial period. Further, the patients taking the krill oil did not report any of the undesirable effects sometimes linked to fish oil, such as “fish burps,” flatulence, diarrhea, or bleeding/vascular complications. Krill oil is also free from the strong fishy aroma associated with fish oil supplements that some people find unpleasant.
That said, krill oil is not suitable for individuals with shellfish or seafood allergies. Since it is from an animal source, it is not an option for strict vegans and vegetarians, and since it is derived from crustaceans, it is not appropriate for people who follow the Kosher dietary restrictions.
By design, the Australian researchers recruited patients with mild to moderate knee OA for this trial, but excluded those with more severe conditions. That decision was based on the view that severe knee OA, “may be beyond the point of improvement with a supplement or may require high doses of NSAIDs that may mask any supplement effect.”
For patients with milder, early-stage OA—in whom there is a possibility to reduce knee pain and improve function, krill oil supplementation is a promising option.
END


