




Eczema is seldom life-threatening, but it can have profoundly detrimental impact on the people it affects. Clinicians who can bring a holistic, root-cause approach to this common condition can make a big difference in the lives of their patients.
“Roughly 20 million Americans have eczema. It’s a huge population. Patients are desperate for help, and very few practitioners are providing holistic, functional dermatology care,” says Julie Greenberg, ND, founder of the Center for Integrative & Naturopathic Dermatology, Los Angeles.
Severe eczema, aka atopic dermatitis, causes significant physical suffering, disrupts sleep, and often leads to social isolation and depression. Some patients find it difficult, if not impossible, to work. That means the disorder can cause long-term economic hardship.

“It’s not just a little rash. It can really impact lives,” said Greenberg in a webinar hosted by Integrative Practitioner. “These patients are motivated, they’re compliant, they really want to get better,” Dr. Greenberg said. One of her severe eczema patients once told her, “If you tell me to eat dirt, I’ll eat dirt.”
Dr. Greenberg, who is also a registered herbalist with the American Herbalists Guild (AHG), has years of experience treating severe skin disease exclusively with diet, lifestyle change, and botanical medicine. Through her Root Cause Dermatology training program she’s teaching other clinicians to do the same. The need for this, she says, is tremendous.
Boiling Over
The word eczema derives from the Greek “Ekzein”, meaning to “boil over.” The very name implies heat, inflammation. And that, says Greenberg, should be the central focus of treatment.
She stressed that chronic skin problems like eczema are rarely just skin problems. In nearly all cases, there are underlying systemic problems that warrant attention. “It is a disease of skin barrier dysfunction, but also a disease of deep systemic inflammation.”
Think of eczema as “leaky skin,” which is directly analogous and often concurrent with leaky gut.
While it is important to quell the obvious symptoms and give patients some measure of relief, it is equally important to identify and mitigate the drivers of inflammation. As with all chronic inflammatory diseases, the specific drivers vary from patient to patient.
Not Just Th2
To effectively treat eczema, you need to start with the pathophysiology says Dr. Greenberg.
The standard immunological view is that eczema is a Th2-mediated disorder. Th2 immune responses are typically triggered by helminths, fungi, and allergens, and mediated by cytokines like IL4, IL5, and IL13.
It is generally true that people with eczema do show Th2 predominance, and many of the drug therapies for eczema, including the injectable biologics, squelch the Th2 response. “Compared with psoriasis, it (eczema) is completely different. Psoriasis does not have a Th2 component.”
But Dr. Greenberg stressed that eczema is not always exclusively a Th2 disease. “It can have a Th1 or Th17 component as well.”
Th1 responses are typically driven by intracellular bacteria, viruses, and protozoa, while Th17 responses are usually driven by extracellular bacteria and fungi at mucocutaneous sites. Some people even show a Th22 pattern, suggestive of tissue inflammation.
In evaluating people with eczema, it’s important to take all these factors into consideration.
Immunological Endotypes
Greenberg cited a 2019 review by Tali Czarnowicki and colleagues that looked at immunological endotypes in diverse populations with atopic dermatitis.
They compared European-American, Asian-American, and African-American cohorts, and found that while all showed Th2 features, the Asian-Americans were more likely to show Th17 responses than European- or African-Americans.
There were also age-related differences: pediatric patients were more likely than adults to show Th17 responses. These are just a couple of the endotype patterns that Czarnowicki discovered. The point is, atopic dermatitis may not be as uniform as we previously thought. This suggests that treatments also need to be individualized and tailored to immunological endotype, rather than simply to lesion severity (Czarnowicki T, et al. J Allerg Clin Immunol. 2019)
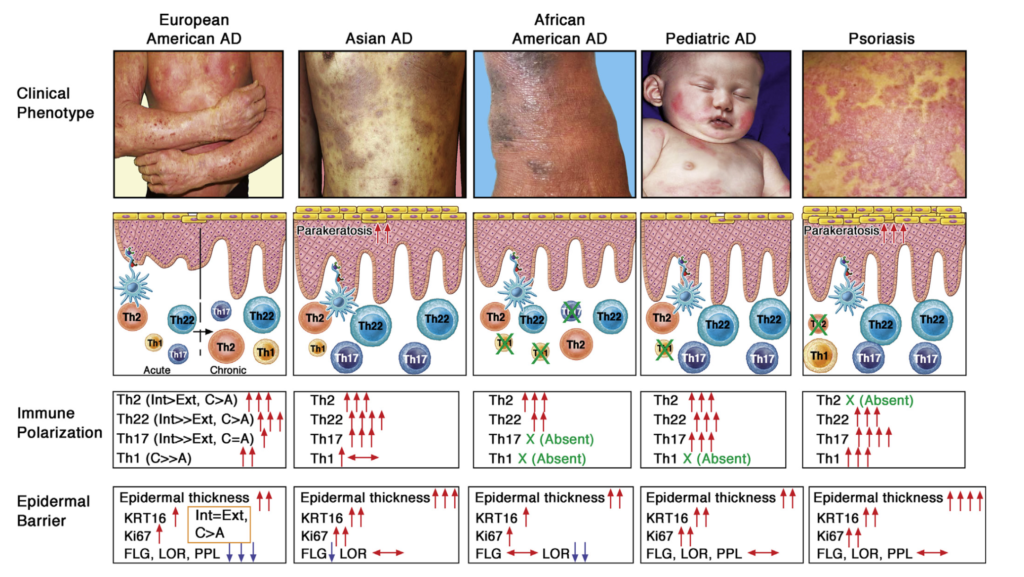
“An attempt to define the patient’s endotype before treatment should be made to optimize therapeutic responses moving toward precision medicine based on the different clinical and molecular disease subsets,” writes Czarnowicki. “Although Th2 axis activation seems to be a universal trait across the AD spectrum, it still might be the case that other or additional cytokine targeting will be highly effective for a particular subset of patients who present a distinct endotype.”
The Role of Food Allergies
Dr. Greenberg called food allergies the “elephant in the room” in eczema. Though it is not accurate to say food allergies ‘cause’ the disease, they certainly can play a role in driving the process and triggering flares.
“It’s important to consider, but strictly focusing on food triggers is less likely to give you strong traction in adults with eczema. Food eliminations can help some people, but it’s not a cure-all.
But again, the impact of food allergies—which can be IgG-, IgA-, or IgE-mediated–varies widely between patients. Age is a factor in this: allergies play a much more prominent role in infants and young children than they do in adults with eczema.
According to Thomas Werfel and Kristine Breuer at the Hannover Medical University, Germany, well over 50% of children with atopic dermatitis experience exacerbations in association with particular foods (Werfel T, Breuer K. Curr Opin Allergy Clin Immunol. 2004).
But adolescents and adults are far less likely to experience food-associated flares. Dr. Greenberg estimated that two-thirds of all adult eczema patients do not show signs of allergy to food or environmental allergens. That’s partly because people tend to outgrow childhood allergies to milk, eggs, wheat, soy, and other common allergens. Further, by the time people reach their 20s and 30s, they’re usually aware of their problem foods, and they tend to avoid them.

“It’s important to consider, but strictly focusing on food triggers is less likely to give you strong traction in adults with eczema. Food eliminations can help some people, but it’s not a cure-all. Try it and see. But if food elimination is not working, not giving total clearance, don’t get stuck. You need to dig deeper.”
Dairy is No Friend
What’s the most common culprit food group? Dairy.
“When patients do experience food-related eczema flares, 75% are due to milk or dairy,” Dr. Greenberg said, adding that when taking a patient’s history, it is really important to ask about all forms of dairy, not just milk.
“If you ask about “milk,” patients will think you mean drinking glasses of milk. They’ll say “no.” But then later you’ll find out that they eat a lot of cheese. So, ask about anything that’s produced by a mammal mamma for a baby, and that includes sheep and goats too.”
Without restoring gut health, it is difficult if not impossible to maintain skin health.
Greenberg says she encourages all her eczema patients to eliminate dairy. They might not all be frankly allergic to it, but as a food category dairy is seldom doing them any good. “I’ve yet to meet an eczema patient for whom dairy is doing any favors. So, I just take it out.” Other common trigger foods are wheat/gluten, eggs, peanuts, and soy.
“Wheat is 50/50. Some patients are sensitive, some are not. Stool testing and organic acid testing will usually show it,” she said. Regarding eggs, the degree to which people experience flares is often “dose dependent.” Most can eat eggs occasionally without flaring, but eating them several times per week or more increases the risk of flares.
For some patients, wine and especially red wine, can be problematic. “It’s high in histamines, and high in yeast. In patients with fungal overgrowth, you don’t want to give more yeast,” Dr. Greenberg said. Further, alcohol converts to sugar which fuels inflammation.
Does Eczema Cause Allergies?
We could also ask whether eczema causes food allergies, says Dr. Greenberg. “It’s a weird way to think about things, but we think that this is likely.”
Food sensitization problems are 6 times more common in kids who have eczema compared with those who do not, according to a study by Tamara Strugar and colleagues (Strugar TL, et al. J Drugs Dermatol. 2019). Generally speaking, the eczema develops first, then the food allergies and sensitivities.
Any type of skin barrier disruption during infancy positively predicts the emergence of food allergies by age 2. Dr. Greenberg noted that kids who have eczema early in life are also much more likely to develop asthma than those without eczema.
Based on a systematic review of 66 separate studies, Teresa Tsakok and colleagues at the St. John’s Institute of Dermatology, London, estimate that one-third of all children with early onset eczema go on to develop food allergies, asthma, or both, later in life (Tsakok T, et al. J All Clin Immunol. 2016). Researchers have described this as the “Atopic Triad.”
Leaky Skin, Leaky Gut
What are the connections? Think of eczema as “leaky skin,” which is directly analogous and often concurrent with leaky gut.
The skin is constantly in contact with the external world, exposed to a host of potentially noxious substances such as environmental toxins, pollen, food allergens, viruses, mites, animal dander, plant irritants, and the like. “They’re outside us. They shouldn’t get in. They shouldn’t reach the dendritic cells. And when the skin is healthy, they don’t get in and the immune system remains calm,” she explained.
Eczematous skin is characterized by breaches in the epidermal barrier. Things that should be on the outside get down into deeper layers where they reach the dendritic cells, and this generates the various types of T-cell responses.
The same thing is happening in the gut. Dr. Greenberg noted that each time we swallow—a phenomenon that happens roughly 2,000 times per day—we are bringing the “outside” world inside the body.
A healthy, well-functioning digestive tract has multiple mechanisms—stomach acid, mucus production, microbiome factors, tight junctions between endothelial cells—for preventing noxious stimuli from entering into the bloodstream and the tissues.
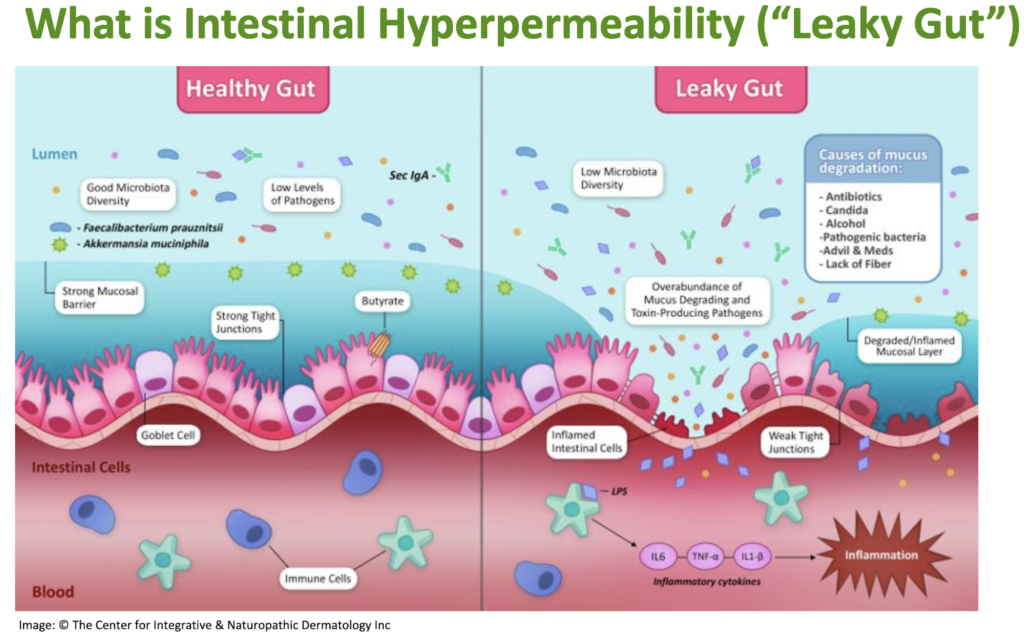
“In a leaky gut, there’s a breach of the mucosal layer and the lumenal contents get in, which is very inflammatory, leading to further breakdown of the mucosal barrier. Things get into the bloodstream that do not belong there. Lipopolysaccharides get through
and activate the dendritic cells, causing the release of IL6, TNF alpha, IL1-beta, which drives inflammation.”
Treat the Gut
Whether the initial barrier breakdown is in the skin or in the gut, the key to long-term resolution of eczema lies in careful assessment and treatment of the latter. Without restoring gut health, it is difficult if not impossible to maintain skin health.
“I test and treat the gut in all my eczema patients,” says Dr. Greenberg. “I run a stool (microbiome) test and an organic acid test on every single patient I see, right before the first visit. As a naturopath, I’m interested in their digestive function, so I look at markers for what’s going in, and what’s coming out. I look at how someone’s extracting and absorbing nutrients from what he or she is eating.”
She says she pays close attention to several key aspects of gut health, including:
- Oral and Nasopharyngeal Microbiome: Though the intestinal microbiome dominates research and popular discussions about probiotics, it is only one part of the overall picture. Many problems begin upstream, with the oral and nasopharyngeal microbiomes. Dr. Greenberg advises checking the oropharynx. Is there evidence of gingivitis? Chronic nasal or sinus infection? Has the patient had extensive dental work? Root canal therapies? All of these factors may play contributing roles in the underlying inflammation.
- Stomach acid production: Many people with eczema are hypochlorhydric. They’re not producing enough stomach acid, which means that potentially problematic microbes that would normally be destroyed in a properly acidic stomach, are getting through to the intestines. The problem is amplified in those who carry Helicobacter pylori, and those on acid-blocking drugs.
- Evidence of dysbiosis: Eczema patients often show overgrowth of certain commensal organisms, an absence of beneficial bacteria, and/or the presence of pathogenic bugs.
Microbiome Factors
A healthy human intestinal tract will show robust populations of Faecalibacterium prauznitsii—an important producer of butyrate—and Akkermansia mucinophila—which eats old mucus and stimulates endothelial goblet cells to produce more mucus.
Eczema patients almost always show low levels of both. That means they’re usually deficient in butyrate, which is produced by F. prauznitsii as it ferments dietary fiber. Butyrate is the preferred fuel of enterocytes, and it also quells inflammation. The absence of A. mucinophilia means the gut is less able to repair and restore its protective mucus layer.
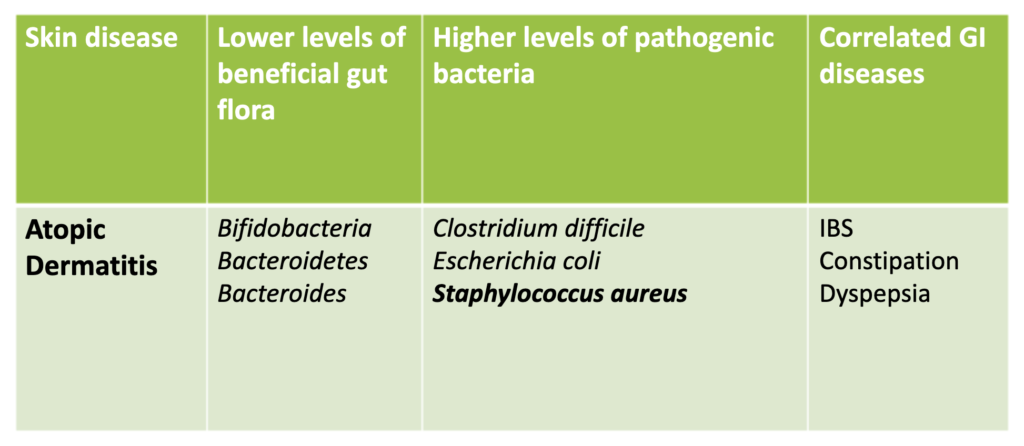
Many eczema patients also show relatively low levels of beneficial organisms such as Bifidobacteria and Bacteroidetes, but overgrowth of Staphylococcus aureus, various species of Streptococcus, Escherichia coli, and fungi like Candida albicans.
These microbiome changes are evident very early in life. Lotte Nylund and colleagues at the University of Turku, Finland, showed that infants with severe atopic dermatitis have far lower levels of butyrate-producing bacteria in their GI tracts than do healthy infants and those with mild AD (Nylund L, et al. Allergy. 2015).
Generally speaking, the severity of atopic disease is inversely correlated with GI microbial diversity, and with the presence of butyrate-producing organisms.
A Role for Probiotics
Given these relationships, it’s reasonable to think that probiotic supplementation could be helpful in treating eczema. Dr. Greenberg says they do have a role, but on their own, they are seldom going to result in complete resolution of skin symptoms, especially in severe eczema.
“I use probiotics, but it’s definitely not the only the only thing,” she said.
Clinical studies are conflicting. The most comprehensive paper on this topic–a 2019 systematic review of 44 separate trials of probiotics in atopic patients–came to a split conclusion: 50% of the studies showed benefits from probiotics, but the other 50% showed no effect (Petersen E, et al. Acta Dermatol Venereol. 2019).
That stalemate is due in part to the extreme heterogeneity of the studies included in the review: probiotic strains, doses, and treatment durations varied widely from trial to trial.
Dr. Greenberg said some of her own patients have been getting good results from a relatively new probiotic product containing live Akkermansia mucinophilia. Made by Pendulum Health, this is the only product on the market providing the live form of this important organism.
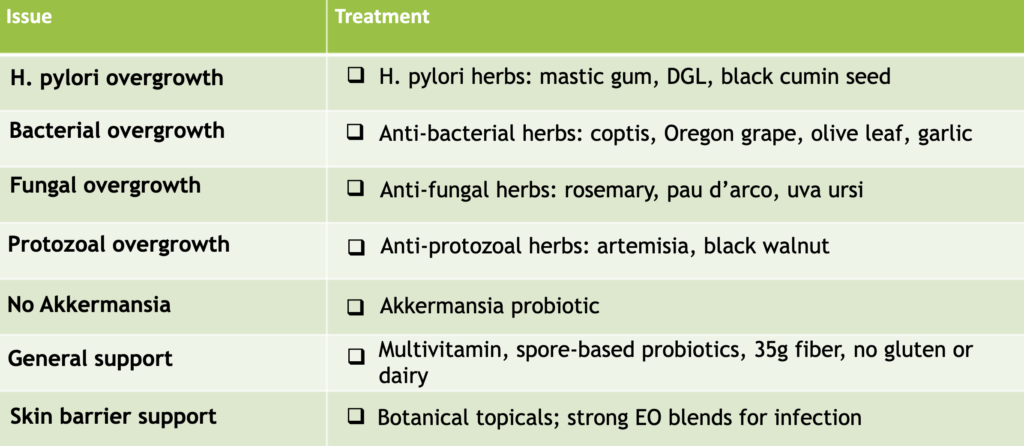
But again, Akkermansia probiotics are not a cure-all. Greenberg said she often uses spore-based probiotics as well. And she insists that her patients get at least 35 grams of dietary fiber per day, either from food, supplements, or a combination of the two. “I make all my patients take a lot of fiber. Most people really lack it in their diets.”
Tackling Candida
Candida is a big culprit in people with eczema.
GI overgrowth of candida shows a statistically significant correlation with IgE antibodies in atopic dermatitis patients (Savolainen J, et al. Clin & Experimental Allergy. 1993). The authors of this study noted that “Severe phases of AD in colonized patients are associated with IgE synthesis against C. albicans.”
When AD patients who do have IgE antibodies to Candida are treated with antifungals, the skin symptoms improve. This was shown 25 years ago, in a study by a team of dermatologists at Hiroshima University School of Medicine in Japan (Morita E, et al. J Dermatol. 1999).
“I find this 100 percent,” said Dr. Greenberg, referring to her own experience treating Candida in people with eczema.
Keep in mind that in addition to triggering a shift from Th1 to Th2 immunological patterns, the presence of fungi like Candida at mucocutaneous sites will also drive Th17 reactions. Many people with leaky gut will show Th17 reactions, and these are associated with autoimmune conditions. It’s important to keep this in mind.
Candida overgrowth is very common among people with eczema. “Get the Candida down, and the skin gets a lot better,” says Dr. Greenberg. She stressed that she treats fungal infections via dietary changes and herbal antifungals such as Rosemary (Salvia Rosmarinus), Pau d’arco aka Lapacho (Handroanthus impetignosus), and Uva Ursi (Arctostaphylos uva-ursi).
H. Pylori: A Hidden Culprit
Be on the lookout for Helicobacter pylori in your eczema patients, says Dr. Greenberg.

Roughly half of all people carry H. pylori, and for many, it seems to cause no harm. This has led some researchers to view it as a benign commensal. But for some people, this bug is highly problematic. It’s association with peptic ulcers, gastritis, and gastric cancer are well-known. Fewer people are aware that it is also linked to skin diseases like rosacea, chronic urticaria, eczema, severe acne, and alopecia areata.
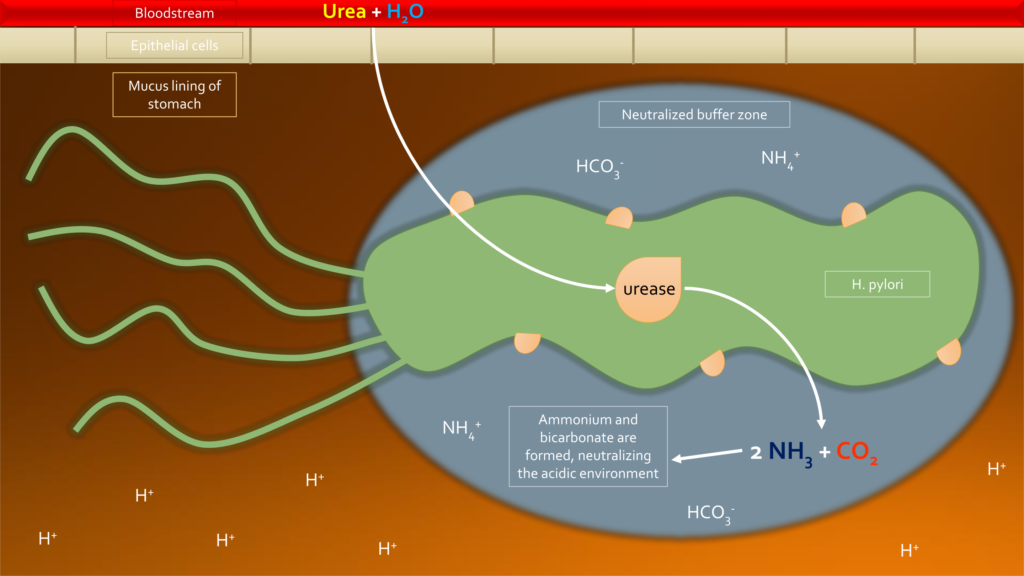
H. pylori can produce lipopolysaccharides and endotoxins, as well as biofilms, all of which can be problematic, especially in people who already have compromised mucosal barriers and systemic inflammation.
It also produces urease and other substances which create a buffer against stomach acid. This allows the organism to live in a very low-pH environment that normally would be utterly hostile for bacteria. In other words, it diminishes one of the body’s primary defenses against noxious stimuli from the outside world. The neutralization of stomach acid also leads to suboptimal digestion, which has downstream consequences.
“Stomach acid signals to the pancreas and gall bladder to produce bile and enzymes. A deficit of stomach acid leads to suboptimal production of enough bile, pancreatic enzymes,” Dr. Greenberg explained. “That’s not good for us.”
This acid-mitigating effect ensures H. pylori’s own survival, and it also enables potentially problematic protozoans like Giardia and Entamoeba to survive the stomach and enter the intestines.
Protozoans are common findings in stool analyses of people with eczema, and these patients almost always have H. pylori.
Are the protozoans always pathogenic? No, but Dr. Greenberg says she errs on the side of treating them as such. Her go-to botanicals for eliminating protozoans are Artemisia and Black Walnut (Juglans nigra). Likewise, she considers H. pylori to be an etiologic factor in eczema, and treats it accordingly, even if the patients do not have peptic ulcers or gastritis. Her preferred herbs for mitigating H. pylori are: Mastic gum, deglycyrrhizinated licorice (DGL), and black cumin (Nigella sativa).
The Ear Infection Connection
There is a strong connection between chronic ear infections and eczema. Dr. Greenberg noted that most children with eczema also have frequent ear infections. And if you ask, you’ll find that many adults with eczema have histories of chronic ear infections in childhood.
The reasons for the association might not be obvious. But embryologically, it makes sense. The bones of the middle ear, and the eustachian tubes develop from the first and third pharyngeal arches which are the developmental foundation of the head and neck, including the pharynx. The eustachian tubes themselves open into the nasopharynx.
This means there’s a fundamental anatomical connection between the ears, the digestive, and the respiratory tracts. We think of them as separate systems, but actually, they are interconnected.
In a recent review paper, Amy S. Graham and colleagues at the Neuroscience Institute, University of Cape Town, South Africa, explored these connections in detail, coining the term “Auditory-Gut-Brain Axis.” They suggest that changes in the gut microbiome, chronic inflammation, and disorders of the ear and of auditory processing, may all be related (Graham AS, et al. Front Neurosci. 2023).
On the patient care level, Dr. Greenberg reported that she’s had a number of eczema patients who experienced complete clearing or at least significant improvement of ear infections after eliminating dairy and wheat as part of a lifestyle program to mitigate the eczema. “I started to advise my ear infection patients to cut out wheat and dairy, even if they don’t have eczema. Many have gotten better.”
Assessing Eczema Patients
In addition to a thorough history and physical exam, Dr. Greenberg’s initial assessment depends on two cornerstone tests: the GI-MAP (Microbial Assay Plus), a PCR-based test to detect the presence of various bacteria, fungi, viruses, worms, and protozoa in fecal samples; and an Organic Acid Test, to assess overall nutrition status, metabolic function, detoxification capacity, and neurotransmitter status.

“Every patient has to do the GI-MAP and the OAT before the first visit. I use these as a baseline. It’s immensely helpful. Depending on the clinical history, and initial evaluation, I might order other tests as well.”
Other potentially useful tests include the DUTCH tests (Dried Urine Test for Comprehensive Hormones); Mold and mycotoxin tests; Hydrogen or methane breath testing for small intestinal bacterial overgrowth (SIBO); Food allergen tests; and specific tests to assess intestinal permeability.
“I use the labs as a roadmap. I know where we’re starting: severe eczema. And I know where we want to go: clear skin. The findings from the labs give clues on where to focus treatment-wise.”
Individualizing Treatment
Given the range of immunological endotypes, microbiome factors, and potential food and environmental triggers that can contribute to the pathogenesis of eczema, an effective treatment program must necessarily be individualized, says Dr. Greenberg. She adds that resolution of chronic eczema takes time, and that she typically shifts the focus of treatment every 2-3 months.
“These patients are motivated, they’re compliant, they really want to get better”
The fundamental goals of treatment are to quell systemic inflammation, eliminate inflammatory triggers, eliminate pathogens, restore a healthy gut, oropharyngeal, and skin microbiomes, and repair damaged skin and gut mucosa.
She stressed that as a naturopathic physician, she does not use prescription drugs, but is able to achieve excellent results with lifestyle modification, dietary changes, food trigger eliminations, herbal antimicrobials, and probiotics.
“You have to go deep. It’s far beyond prescribing tubes of steroids or Th2 response inhibitor drugs. That’s all just system suppression. You push down the Th2 response, you push down the inflammation. But you’re not really finding and treating the root causes. You can’t just treat from the outside in, you have to also work from the outside in.”
She added that the general approach she takes with eczema patients will often work well for those who have psoriasis and other chronic skin disorders.
END


