




Prevalence of eosinic esophagitis is rising the US. Though seldom life-threatening, this condition is highly burdensome for those affected. Over the long term, it can have detrimental impact on nutritional status and overall health.
Fortunately, EoE is often responsive to dietary interventions if carefully implemented, said Bethany Doerfler, MS, RD, at the 2023 Integrative Healthcare Symposium in New York City.
Doerfler, a member of the Functional Bowel and Neurogastromotility Team at Northwestern University Medical Center, Chicago, is a prominent advocate for diet-based management of eosinophilic esophagitis (EOE) and other allergic and inflammatory gastrointestinal conditions.
“Diet therapy works in EoE. Multidisciplinary care will improve patient outcomes,” she told IHS attendees.
“What we’re talking about here is a Th-2 type pathway, like asthma, but in the esophagus.”
—Bethany Doerfler, RD, Northwestern University
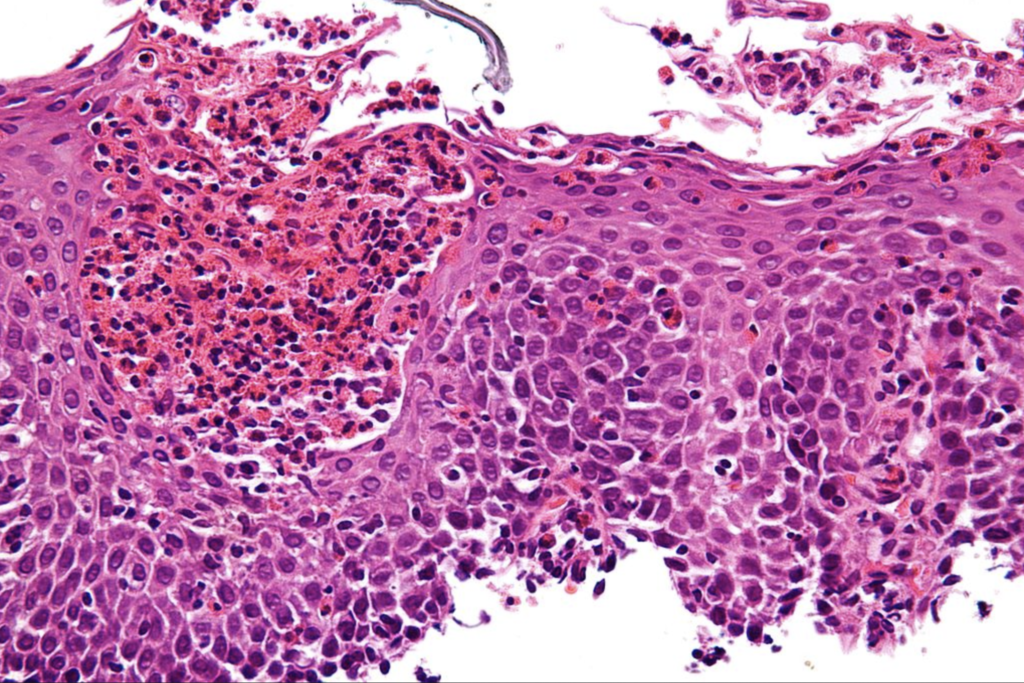
EoE is characterized by infiltration of large numbers of eosinophils into the soft tissue of the esophagus, which is normally free of these cells. This typically triggers inflammation and tissue damage that manifests as heartburn, abdominal or chest pain, difficulty swallowing, and food impaction. If it persists, it raises the risk of more serious esophageal problems like strictures and achalasia.
Since EoE makes swallowing uncomfortable and difficult, patients often limit their food intake, which can compromise nutritional status over time.
Rising Prevalence
Once considered rare, EoE is actually more common than many clinicians realize. The prevalence appears to be increasing in both children and adults. Several recent epidemiological studies have shown that prevalence has doubled over the last two decades (Kumar S, et al. Pediatr Research. 2020, Kamat S, Am J Gastroenterol. 2021).
Researchers at the Mount Sinai Center for Eosinophilic Disorders, Icahn School of Medicine, New York, calculated EoE prevalence in a cohort of roughly 20 million enrollees in commercial or Medicare insurance plans from 2015 to 2018.
They found that the number of new EoE diagnoses rose from 16,980 in 2015, to 22,978 in 2018, a 35% increase. The annual prevalence rate increased from 79 cases per 100,000 enrollees in 2015 to 117 per 100,000 in 2018 (Kamat S, Am J Gastroenterol. 2021).
When they stratified the data by 5-year age increments, they found that risk was highest in people between 35 and 44 years. There was also a clear gender disparity. Across all ages, EoE prevalence was consistently higher in males versus females. In 2018, the rate was almost 2-fold higher for males versus females (151 vs 86 per 100,000 enrollees).
Once considered rare, the prevalence of EoE appears to be increasing in both children and adults. Several recent epidemiological studies have shown that prevalence has doubled over the last two decades.
The rise is due in part to greater clinician awareness and better diagnostic accuracy. But there also seems to be an objective increase in the number of people affected.
EoE & Food Allergies
EoE is defined as a chronic, immune-mediated condition characterized by eosinophil-predominant inflammation which shows up histologically as ≥15 eosinophils per high-power field in the esophageal mucosa.
“Eosinophils should be in the bloodstream. But they can migrate into the soft tissue of the esophagus and sometimes the stomach as well. They ramp up inflammatory pathways and wreak havoc,” explained Doerfler, at the IHS. “Eosinophils fight off foreign invaders, but that process often goes awry. In addition to eosinophilic forms of asthma, there are also eosinophilic GI disorders and EoE is one of them.”
According to the American Gastroenterological Association, EoE is caused by a chronic T-helper type 2 immune hypersensitivity response to one or more food allergens. There’s a large overlap between EoE and other types of allergic disease including asthma, eczema, and seasonal or environmental allergies.
In a new study of 341 patients with longstanding EoE, 88% had one or more atopic or allergic comorbidity at the time they were assigned for treatment with either a placebo or subcutaneous dupilumab (a monoclonal antibody recently approved for treating type 2 inflammatory diseases. The three most common comorbidities were allergic rhinitis, non-food allergies, and food allergies.
The study, by Marc E. Rothenberg, MD, PhD, at the Cincinnati Center for Eosinophilic Disorders, was presented as a poster at the American Academy of Allergy, Asthma & Immunology’s 2023 annual meeting, but has not yet been published. The findings add to the evidence documenting the strong relationship between EoE and other inflammatory diseases.
Endoscopy is Key
“What we’re talking about here is a Th-2 type pathway, like asthma, but in the esophagus,” Doerfler explained.

“When the eosinophils infiltrate the esophagus, the surface mucosa develops very distinctive concentric rings, furrows, tracks, and white spots filled with eosinophils. It is quite visible on endoscopy.”
Many symptoms of EOE are common to other upper GI conditions, which can make it difficult to diagnose based on clinical complaints alone. The most distinctive symptom is the sensation of food gets stuck when one is swallowing. If a patient says something like, “The food feels like it’s slow to go down,” that’s a major red flag for EoE. If it’s something the patient experiences frequently, make a referral for an endoscopic evaluation to find out what’s going on, Doerfler advised.
“We know that the sooner we can diagnose (EoE) and intervene, the more likely we are to minimize risks, especially for things like strictures.”
The Big Six
Pharmaceuticals can sometimes be helpful in severe EoE. Many gastroenterologists consider oral corticosteroids to be the first-line drug options for these patients. Some also prescribe proton pump inhibitors for those who experience acid-mediated GERD in addition to EoE. Last year, the FDA approved dupilumab (Dupixent) for treatment of EoE, making it the first drug specific for this indication.
But all of these pharma options have downsides, and none of them are truly curative. Patients who start on drug therapies without dietary changes are very likely to experience a return of symptoms if they stop the drug treatment.

The real key to managing EoE, says Doerfler, is to identify and eliminate the food or foods that provoke the eosinophilic inflammation. Fortunately, in the vast majority of cases, that comes down to just one or two very common foods.
“First focus on the ‘Big Six’ allergenic foods: dairy, wheat/gluten, soy, eggs, tree nuts/peanuts, and fish/seafood,” she said, adding that EoE patients seldom need to follow extreme, long-term, elimination diets.
In 2006, Amir Kagalwalla and colleagues at Northwestern studied the impact of a six-food elimination diet (SFED) for six weeks in children with EoE and found that 74% improved both clinically and histologically. Though an amino acid-based elemental diet gave a slightly higher overall response rate, the SFED was far easier for families to implement, and much less costly (Kagalwalla A, et al. Clin Gastroenterol Hepatol. 2006).
Several subsequent studies have confirmed the efficacy of the SFED approach to treating kids with EoE.
In a large majority of the patients, only one food or food group triggered a resurgence of EoE symptoms and histological signs. In 24%, there were two trigger allergens identified. Only 4% had 3 allergens. That’s good news from a compliance perspective.
More recently, the Northwestern group replicated these findings adults, Doerfler told IHS attendees. “As we collected more data, we found that 65-85% of patients have just one or two foods they’re allergic to. Dairy and gluten are the two most common ones. Eggs, and soy are third and fourth.”
Doerfler and her colleagues recently completed an outcomes analysis of 213 EoE patients who underwent SFEDs and food reintroductions. This is the largest EoE cohort to be tracked through the complete SFED/reintroduction process.
One hundred fifteen patients (54%) showed histological responses, indicated by fewer than 15 eosinophils per high-power field, after an initial six-week SFED; 77% of these responders had meaningful symptom improvement as well (Zalewski A, et al. Am J Gastroenterol. 2022).
Of the 82 patients who did not respond to the initial SFED, 26 (32%) undertook a second round. Of these, 12 (46%) had full or partial responses to the repeat SFED.
The Northwestern researchers were able to run food reintroduction trials, with endoscopic evaluations after each food was reintroduced, in 78% of the patients who showed improvement on the SFED. They found that most common problem food group was dairy, which triggered EoE recurrence in 37% of those retested. This was followed by: wheat (26%), soy (13%), egg (10%), nuts (6%), and seafood (4%).
In a large majority of the patients (69%), only one food or food group triggered a resurgence of EoE symptoms and histological signs. In 24%, there were two trigger allergens identified. Only 4% had 3 allergens.
That’s good news from a long-term compliance perspective.
“Elimination diets stress people out,” Doerfler says. “The more things you have to eliminate, the harder it is. People with multiple food allergies tend to want to go with drug-based medical therapies rather than diet therapies because these diets are often too difficult to maintain over long term.”
If it’s just one or two food groups, even if they’re big ones like dairy, many people are willing to modify their eating habits rather than seeking a pharmaceutical fix, she added.
Guidance Improves Outcomes
But even if it’s just one food group that proves problematic, changing dietary patterns can be challenging. It’s no small thing to entirely eliminate all dairy products, or all gluten-containing foods from one’s culinary routines.
For example, it is pretty easy to avoid eating wheat-based baked goods, but most people don’t realize that things like ice cream, salad dressings, and canned soups or sauces often contain wheat-derived ingredients. Likewise, patients may be diligent about not eating fish, but not realize that there are sometimes fish-based ingredients in things like Worcestershire sauce, barbecue sauce, or gelatin.
That’s where a multidisciplinary dietitian/nutritionist coaching model becomes extremely valuable.
In a new and comprehensive review on the practical implementation of diet therapies for EoE, Joyce Chang, of the University of Michigan’s Department of Internal Medicine, writes that, “Despite several prospective trials demonstrating the efficacy of dietary therapies, successful clinical implementation is hampered by the need for a multidisciplinary approach including dietitian support and provider expertise.”
Unfortunately, most physicians do not have easy access to nutrition professionals who can guide patients on the practical nuts and bolts of changing their diets.
In their paper, Chang and her colleagues note that, “Although many patients may desire a dietary approach to EoE, making it a tenable and positive experience can be as challenging when deciding to start the diet.”
To help fill the gap, their review includes several detailed but patient-friendly guidelines and handouts to help with implementation of empirical elimination diets, food reintroductions, and long-term dietary shifts to minimize risk of EoE recurrence.
During her talk at IHS, Ms. Doerfler emphasized the importance of maintaining food variety and nutrient density for EoE patients making dietary changes. “When you eliminate a staple food, make sure you’re finding things to replace it, things that have enough texture, enough variety of temperatures, and diversity of nutrients. Replace the eliminated foods with healthier alternatives.”
END


