




Since the Spring of 2020, roughly 200 million Americans have had Covid-19. That’s an estimated 60% of the country’s population. Worldwide, the number is around 700 million.
For many, the acute infection was just the beginning of a long, bewildering odyssey of illness.
With Covid-related admissions to US hospitals now under 1 case per 100,000 population, the focus for most clinicians has shifted from preventing and treating acute infections to the challenging task of managing Long Covid, as this post-viral syndrome is known.
Government agencies and medical organizations have yet to reach consensus on formal definitions of Long Covid, and there is considerable debate about its prevalence and its risk factors. But by any accounting, it is a significant public health problem.
According to the World Health Organization, up to 10% of all people who’ve had Covid have persistent symptoms three months (90 days) or more after acute infection. Roughly 2% still have symptoms at 12 months. The Centers for Disease Control defines Long Covid as the presence of symptoms 30 days post-acute infection. By that definition, one in five US adults have (or have had) Long Covid.
Recent reports suggest that incidence may be on the wane. According to a national survey of more than 60,000 individuals by the Census Bureau and the National Center for Health Statistics, the number of Covid patients who report long-term symptoms declined from 35% to 28% between June 2022 and January 2023.
That’s a positive signal, but on a population basis, the Long Covid numbers are still massive. And official figures may underestimate the problem, because cases only show up in epidemiological databases when practitioners diagnose them and code for them properly. Given that many Long Covid symptoms overlap other disorders, a lot of cases may not be properly logged.
A Chaotic Situation
There are upwards of 200 distinct symptoms linked with the post-Covid syndrome, and they can affect nearly every organ system. Though sometimes disabling, they’re often diffuse and episodic, appearing, disappearing, and reappearing in seemingly random manner. And unlike the acute infection, there is no definitive “yes or no” test for Long Covid.
In May, the National Institutes of Health published the first data from the Researching Covid to Enhance Recovery (RECOVER) project. Based on records from nearly 10,000 adults, the paper is NIH’s first attempt to formally define the post-Covid syndrome, catalog its most common symptoms, identify who’s at risk, and provide direction for future clinical guidelines and research projects.
On a practical level, though, RECOVER offers little to help practitioners right now.
For patients, questions about the formal definition are academic: they simply know that their health cratered after having Covid. They want help, and they have trouble finding it.
A Coherent Framework
Over the last year, a working group of functional medicine practitioners came together to review the world’s literature, compare clinical experiences, and lay groundwork for a comprehensive therapeutic approach to Long Covid.
“The five pathophysiological drivers give us points of orientation for treatment”
–Patrick Hanaway, MD
The resulting 90-day Post-Viral Recovery Program (PVRP), developed under the aegis of OvationLab and ANDHealth, is a major step toward bringing clarity to a confusing situation. It creates a set of multimodal protocols for assessing and treating patients, and provides a coherent framework for further research and refinement.
The 10-member PVRP working group was directed by OvationLab’s Laurie Hofmann, MPH, and included Patrick Hanaway, MD, Kara Parker, MD, Michael Stone, MD, and Kristine Burke, MD.
The group defines Long Covid as “diverse symptoms of new, returning, or ongoing health problems…after an acute Covid infection.”
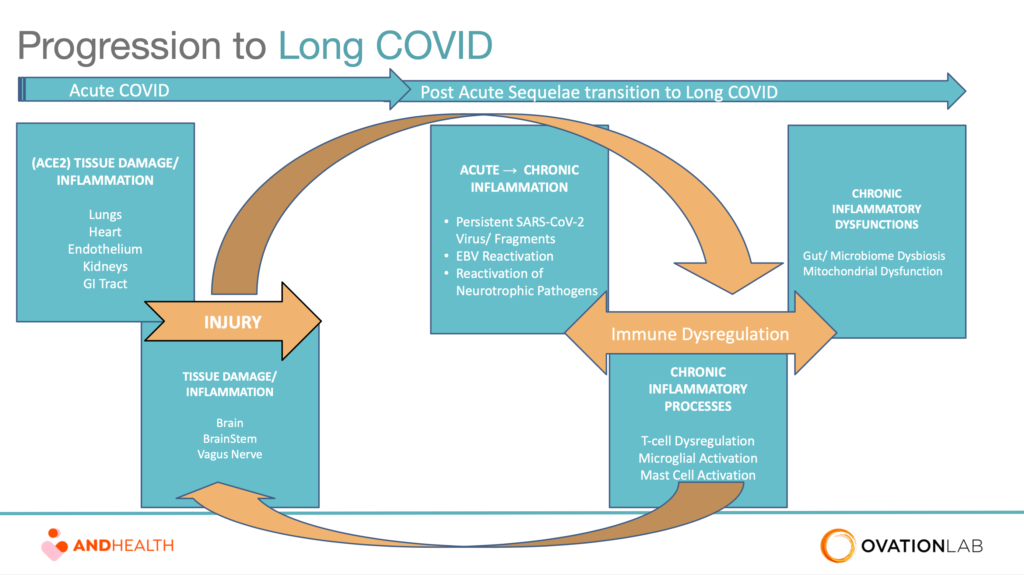
The protocols they developed are centered around the core observation that there are five main physiological drivers underlying the syndrome and its myriad manifestations:
- ACE2-mediated tissue damage
- Viral persistence
- Chronic inflammation
- Microbiome dysbiosis
- Mitochondrial dysfunction
These basic processes are inter-related, and often concurrent (Fig.1). For example, ACE2-mediated tissue damage in one or more organs can trigger chronic, systemic inflammation. Likewise, the presence of persistent viral particles drives immune system dysregulation which feeds the inflammatory cascade. All of the above can disrupt the gut microbiome, resulting in dysbiosis, which adds to the symptom burden.
“The five pathophysiological drivers give us points of orientation for treatment,” says Hanaway, formerly the chief medical education officer of the Institute for Functional Medicine, and founding medical director of the Cleveland Clinic Center for Functional Medicine. He and other Working Group members described the PVRP principles and protocols in a series of three free webinars sponsored by ANDHealth and supported by all of the major functional and integrative medicine education organizations.

“If there’s ongoing tissue damage, we can treat it. If there’s evidence of viral persistence, can we identify the pathogen or pathogens and focus there. If there’s chronic inflammation, we need to define what’s out of balance and take steps to rectify that. Same for the microbiome. And then there’s supporting the mitochondria. These factors all overlap, you can’t just focus on one aspect because they’re all inter-related.”
Working group members recognized that Long Covid shares features with other post-viral syndromes, and that exposure to SARS-CoV-2 often reactivates latent sequestered viruses like EBV, Herpes, and Varicella. Though Long Covid has its own unique characteristics, lessons from post-acute EBV, chronic fatigue, other coronavirus-related diseases, and even Lyme disease, have relevance in this context.
Who’s at Risk?
“We know that people who had more severe SARS CoV-2 infection are more likely to get long Covid,” says Dr. Hanaway. “However, we find that about two-thirds of those 2 million-plus people who have Long Covid actually had mild cases of acute SARS CoV-2.” That’s in part because, statistically, far more people had mild versus severe primary infections. The point is, long term problems often develop in people who had mild initial infections.
Obesity, diabetes, metabolic syndrome, and/or cardiovascular disease raise the risk of Long Covid, as does having a history pre-Covid CFS or other post-viral syndromes.
“If we talk to people and get their clinical histories, we can predict who’s going to get Long Covid with 95% accuracy.”
–Patrick Hanaway, MD
In 2022, researchers at the Institute for Systems Biology published a study looking at potential predictive factors for Long Covid in a cohort of 309 patients. They identified four factors–type 2 diabetes, presence of SARS-CoV-2 RNAemia, Epstein-Barr virus viremia, and presence of specific auto-antibodies as highly predictive (Su Y, et al. Cell. 2022). They also found that patients with severe post-Covid GI problems, show a unique expansion of cytotoxic T-cells measurable during the acute phase of illness.
All that said, roughly one-third of people with Long Covid have no pre-existing conditions or major risk factors at the time of primary infection.
Assessing Long Covid
There are no definitive tests for Long Covid. The Working Group says practitioners can rule out other potential etiologies and concerns from the following basic lab tests: Complete blood count (with differential); Sedimentation rate, Comprehensive metabolic panel; D-dimer; Fibrinogen; high-sensitivity C-Reactive Protein, Vitamin D, Thyroid hormones.
Viewed in context of a patient’s history and timeline, these tests can tell a lot about the patterns of tissue damage, pathogenic reactivation, inflammatory and autoimmune processes, dysbiosis, and mitochondrial function.
Several research groups contend there are distinct “endotypes” or “immunophenotypes” of Long Covid, identifiable by particular cytokine profiles, autoantibodies, and cellular activation phenotypes. In a landmark 2021 paper, Proal and VanElzakker propose that lab testing can predict which patients will likely have clotting and vascular problems, or impairment of brain and vagal nerve function, or viral reactivations, or microbiome dysregulation (Proal AD, VanElzaker MB. Front Microbiol. 2021).
Virologist Akiko Iwasaki and colleagues at Yale School of Medicine showed that by measuring cytokines and markers of cellular activation, they could predict 96% of Long Covid cases in a cohort of 215 individuals. (Klein JB, et al. MedRxiv. 2022).
According to the PVRP Working Group, immunophenotyping may be valuable for research, but it is seldom needed for routine patient care.
Assessing Functional Status
“If we talk to people and get their clinical histories, we can predict who’s going to get Long Covid with 95% accuracy. We don’t need all of the sophisticated immunophenotyping. It won’t really change what we’re going to do,” says Dr. Hanaway.
Lab data needs to be viewed in the context of a patient’s symptom patterns and functional status. The PVRP Working Group advocates routine use of the PROMIS-29 (Patient Reported Outcomes Measurement Information System), through which patients can self-assess seven key domains–pain, fatigue, physical function, sleep, anxiety, depression, and social wellbeing—with simple point-rating scales.
The Post-Covid-19 Functional Status Scale (PCFSS), a tool developed 3 years ago by Dutch researchers, is also helpful. It uses 0-4 rating scales to gauge the impact of Covid-related symptoms on activities of daily life.
Make sure to evaluate exercise tolerance, Hanaway added. Movement is vital for restoration of health, but it needs to be carefully tailored to a patient’s abilities and functional status. Too much can be as problematic as too little.
ACE2-Mediated Tissue Damage
All five drivers play a role in the pathogenesis of Long Covid, to varying degrees. But ACE-2 mediated tissue damage is, arguably, the most central to the disease process.
SARS-CoV-2 can enter any organ containing tissue that expresses ACE2 receptors. This means the heart, liver, pancreas, kidneys, spleen, brain, and tissues throughout the GI tract are vulnerable to viral invasion, inflammation, and damage.
Virally-induced tissue injury leads to immune system dysregulation, which causes further tissue damage. “It’s a feed-forward process,” says Dr. Hanaway.
SARS-CoV-2 can enter any organ containing tissue that expresses ACE2 receptors. This means the heart, liver, pancreas, kidneys, spleen, brain, and tissues throughout the GI tract are vulnerable to viral invasion, inflammation, and damage.
According to Harry Crook and colleagues at the Imperial College, London, that simple fact goes a long way in explaining the diversity of Long Covid symptoms (Crook H, et al. BMJ, 2021). (Fig 2). A 2021 study of 201 people following acute Covid showed that 66% had MRI evidence of damage in the heart, liver, pancreas, kidneys, or spleen 4 months after infection. Many had multi-organ involvement (Dennis A, et al. BMJ Open. 2021).
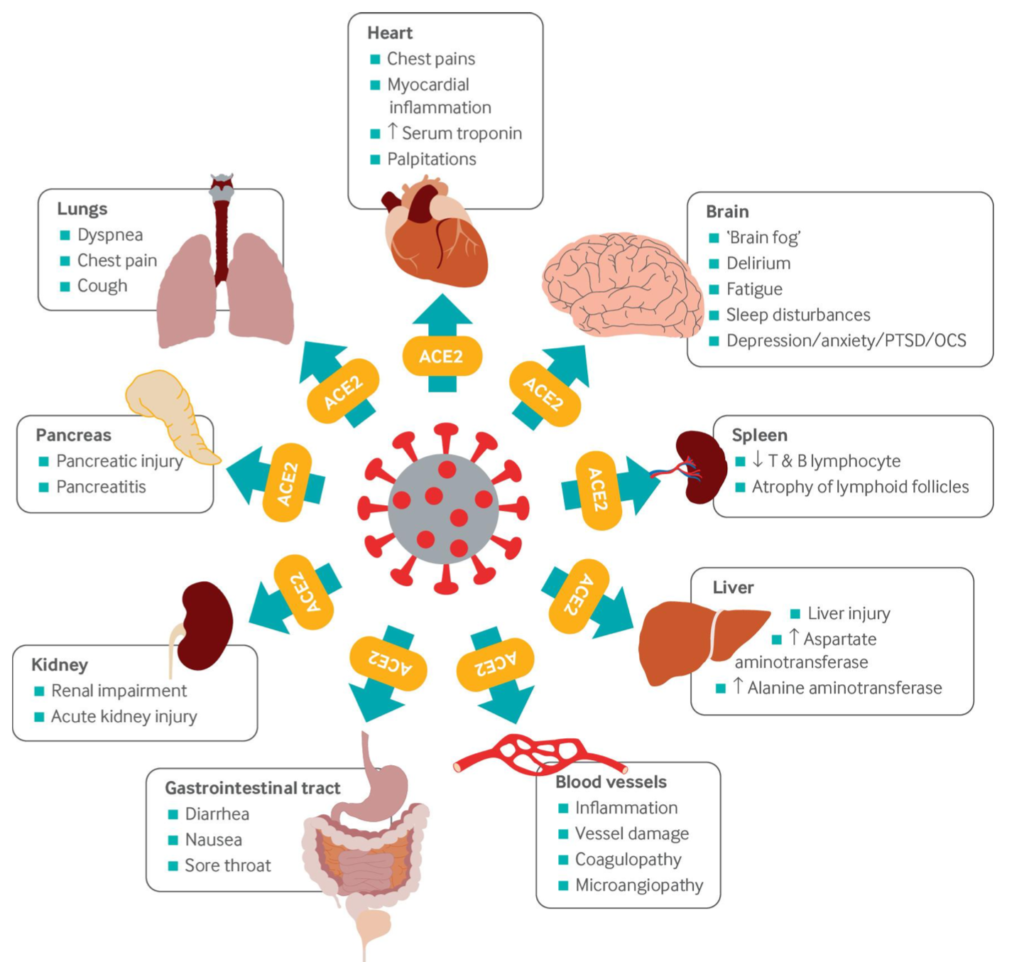
In an excellent review article, Malaysian researchers noted that in the brain, the brainstem region shows the highest density of ACE2 receptors. Viral damage to the brainstem worsens acute Covid, and may underlie longer term neurological and cognitive changes (Yong SJ, Infect Dis (Lond). 2021).
Neuroinflammation may be triggered directly by the virus, or it may be secondary to generalized systemic inflammation, said Dr. Hanaway. It accounts for many of the common symptoms that patients experience: brain fog, sleep disturbances, chronic distress, and anxiety.
The myocardium, which expresses high levels of ACE2, is also vulnerable. In a study of 79 Covid survivors, 29% showed radiological evidence of ventricular remodeling (Moody WE, et al. J Am Soc Echocardiog. 2021). Persistent cardiac symptoms like chest pain, palpitations, and tachycardia are common Long Covid.
So far, there is no evidence of long-term sequestration of whole SARS-CoV-2 virus in human tissue. But researchers have identified a number of specific viral protein fragments that hang around long after the acute illness phase. These can trigger and perpetuate inflammatory responses.
Treating Long Covid
There’s no simple “magic bullet” treatment for Long Covid. Restoring health in the wake of SARS-CoV-2 requires a carefully-tailored, long-term, multimodal approach that includes diet and lifestyle changes, attention to sleep hygiene and stress mitigation, movement and exercise, and intensive nutritional support.

“Changing lifestyle and helping people optimize it in the post-Covid context is not just about treating the Covid-related symptoms. It’s about preventing future harm and future chronic disease,” said Kara Parker, MD, of Hennepin Healthcare, Minneapolis, who is a member of the Working Group. “There’s no downside to helping people improve their lifestyles.”
During the PVRP webinars, which had several thousand physician attendees, Dr. Parker reviewed the key lifestyle facets of the PVRP:
Food & Nutrition: Plant-based, colorful, and minimally processed are the watchwords for good nutrition following Covid. The PVRP nutrition program is built around the Whole30 plant-based program, which Dr. Parker described as “simple and well-resourced.”
The plan provides patients with grocery guides, shopping lists, meal planning tools, plant-based recipes, and tips for navigating the inevitable the ups and downs of energy levels.
Citing a six-country study of nearly 3,000 healthcare workers that looked at the impact of various diet patterns on Covid severity, Dr. Parker noted that those who had plant-based diets prior to infection had a 72% lower rate of hospitalizations and deaths. Those who were primarily plant-based but also included fish had a 50% reduction, compared to those who routinely consumed a lot of meat, processed foods, sugar, alcohol.
In general, plant-based diets reduce HbA1c, increase insulin sensitivity, lower total and LDL cholesterol, improve mood and motivation, downregulate inflammation, reduce BMI, and improve the gut microbiome. All of the above will likely improve the health status of someone dealing with long Covid.
The Working Group chose Whole30 because it simplifies plant-based nutrition. There’s a strictly vegetarian version, and one that includes some animal protein, giving patients the option based on their preferences and nutritional needs.
In general, the Working Group advises:
- Eliminating processed foods and sweetened beverages as much as possible
- Time-restricted eating, for those who can tolerate it
- Low-glycemic meals, to reduce post-prandial glucose surges and inflammation
- Increasing intake of lactofermented foods, to rebuild the microbiome. The exceptions here are patients whose symptoms are suggestive of mast cell dysregulation. Thse patients should avoid foods that trigger histamine release. This includes most fermented foods, aged cheeses, and leftovers of all sorts
- Increasing intake of herbs and spices for flavor and medicinal effects. For example, rosmarinic acid in rosemary, thyme, and other herbs, can help rebuild depleted ACE2 receptors.
“Sleep Snacks”: Circadian rhythm dysfunction, combined with the neuroinflammation caused by the virus, aka “Coronasomnia,” is rampant these days, said Dr. Parker. It can cause blood brain barrier leakage, which creates a feed-forward cycle of more sleep disruption and further circadian dysregulation.
“With sleep, both quantity and quality matter. Any way that we can help patients improve their sleep hygiene and their deep restoration time, will be important.”
One helpful way to do this is to teach patients about ultradian rhythms—the cyclical ebbs and flows of energy that naturally occur over the course of a day—and to work with these cycles rather than fighting them and “pushing through.” Periodic “sleep snacks” during the day can be extremely helpful for people who don’t sleep well at night.
Ultradian breaks need not always be full-on naps. Standing and stretching, yoga postures, walking outdoors, non-caffeinated herbal teas, engaging with a friend or pet, drawing, journaling, reading something enjoyable offscreen, or just giving the mind time to wander, can all be highly restorative.
Regarding nutraceuticals for sleep, the Working Group recommends melatonin when appropriate. Not only does it help reset circadian rhythms, it prevents peroxidation of cardiolipin in mitochondrial membranes. Given that mitochondrial dysfunction is a hallmark of Long Covid, this effect would have obvious benefit for these patients.
Exercise: “Movement is certainly a pillar of healing from Long Covid. But you have to be careful in how you message this. People know this, and they want to move, but oftentimes they have severe post exertional malaise, or POTS (postural orthostatic tachycardia), or orthostatic hypotension, and movement in the way they used to move is not an option,” says Dr. Parker. For some, even minor exertion can result in days-long fatigue and symptom relapse.
Still, some activity is better than none. The key is to tailor activity to the patient’s current energy level, and progress slowly. “Make goals that are attainable for each patient accommodating the new limitations. Be aware that some patients may feel a lot of grief over the loss of their previously high functional levels. It can be a big, big loss.”
Group Visits: A group visit model enables practitioners to efficiently scale their Long Covid care to help more patients, while simultaneously providing patients with much needed social and emotional support. “For people experiencing Long Covid to be with other people who understand them, and what they’re going through is fantastic,” says Dr. Parker who’s worked with hundreds of patients in groups over the last 3 years.
She runs the groups in 7-week series, that includes in-person and virtual visits. The latter, she says are really helpful for these patients, many of whom “already have a medicalized life, and are often going to lots of visits.”
“Movement is certainly a pillar of healing from Long Covid. But you have to be careful in how you message this. People know this, and they want to move, but oftentimes they have severe post exertional malaise, or POTS, or orthostatic hypotension, and movement in the way they used to move is not an option,”
–Kara Parker, MD
Targeted Supplementation
Dietary improvements and other lifestyle changes go a long way in improving someone’s general health status post-Covid. But most patients with Long Covid will require a period of intensive supplementation aimed at mitigating the physiological drivers of the condition.
In developing their supplement recommendations, the PVRP Working Group made an exhaustive search of the global literature to find safe, evidence-based botanicals and nutraceuticals that would be relevant for and accessible to Long Covid patients.
“We found ourselves needing a curated suite of nutritional product solutions that were targeted at the five main drivers of Long Covid: ACE2 mediated damage/tissue damage; viral persistence; chronic inflammation; mitochondrial dysfunction; and microbiome/dysbiosis,” said Kristine Burke, MD, a member of the Working Group.

“We’re not promoting specific brands necessarily. But the ones on the list, we found data to support the use of each of them to target one or more of the five key drivers,” she said during the PVRP webinars.
The protocols are divided into two sets: Foundational Supplements that include basic vitamins, minerals, omega-3 fatty acids, antioxidants, and products to optimize mitochondrial function; and “Specialty” Supplements, which specifically target the five drivers.
“We found ourselves needing a curated suite of nutritional product solutions that were targeted at the five main drivers of Long Covid: ACE2 mediated damage/tissue damage; viral persistence; chronic inflammation; mitochondrial dysfunction; and microbiome/dysbiosis.”
–Kristine Burke, MD
The latter list includes some new and unique products, like Tollovid (Todos Medical)—a compound derived from Lithospermum erythrorhizon, an Asian medicinal plant. It binds the 3CL protease that many RNA viruses produce to cleave their RNA. In so doing, it inhibits viral replication, thus targeting the Viral Persistence driver.
Another new product called ITIS (Return Healthy) is a combination of anti-inflammatory herbs including Scutellaria (Skullcap), Curcumin, Boswellia, and others. It is unique in that it crosses the blood-brain barrier, meaning that it will help with the cognitive impairment and mood disturbances often seen in Long Covid. It also mitigates inflammation, reduces pain, and improves joint and muscle function.
Dr. Parker says that addition of the PVRP supplement regimens can make a major difference over lifestyle changes alone. “I’ve seen this over and over again.”
But it is important to recognize that adherence to this 90-day program requires a strong commitment. “Supplementation is, in fact, a lifestyle change for many patients.”
Origins of the PVRP
OvationLab, a consulting firm focused on developing products, services, protocols, and technologies in the functional and integrative medicine field became the hub of the protocol development process because its leaders—Laurie Hofmann, Tom Blue, and Andie Crosby are well-known and well connected in the functional medicine space, and because they began doing surveys on the impact of Covid early on in the pandemic.
Hofmann told Holistic Primary Care that she and her colleagues saw an urgent need for a comprehensive, systematized, “root cause” approach to the evaluation and treatment of Long Covid.

ANDHealth, a private company that specializes in bundling condition-specific, root-cause care services for chronic disease reversal, played a catalytic role in the evolution of PVRP. ANDHealth launched in 2021 and is funded in part by the venture capital arm of the American Medical Association. It provides its services to patients across the socioeconomic spectrum
Ovation and ANDHealth already had a working relationship when, in late 2021, AND provided funding to assemble the Long Covid working group.
Early in 2022, the team convened what Hofmann called a “social listening” study, analyzing over 1 million social media conversations about Covid and its post-acute sequelae, to find out what people were experiencing, what were their greatest concerns, and what were their biggest unmet needs.
Simultaneously, the 10-member clinical working group was gathering and assimilating the scientific literature on the post-Covid syndrome, sharing their own patient care experiences, and studying the prevention and treatment recommendations developed earlier in the pandemic by medical organizations like the Institute for Functional Medicine.
From this process emerged the identification of the 5 primary physiologic drivers, a standardized set of outcomes measures, the lifestyle recommendations, and the 90-day treatment protocol which are the basic components of the PVRP.
Outcomes Research
Research is of paramount importance to Ovation and the members of the Working Group. To that end, the group collaborated with National University of Naturopathic Medicine to establish a REDCap patient registry to track and quantify functional outcomes in cohorts of patients as they progress through the PVRP protocols.
Last December, the PVRP group began enrolling its first patients, notably Dr. Parker’s group visit patients at Hennepin Healthcare, and from numerous clinical practices around the country.
The goal is to evaluate patients at 30, 60, and 90 days into the PVRP program, using the PROMIS-29 and post-Covid Function Scale (PCFS). The initial patient intake process is quite thorough, and gathers complete history, lab values, and timeline information, though Parker said the forms are “specifically written for people with low energy and brain fog.”
As of April 2023, more than 100 patients have enrolled in the registry, and the first cohort has completed the 90-day treatment protocol. The initial outcomes data will help the Working Group revise and refine the protocols. They will also provide the basis for a series of case studies from the project, the first step toward a full-scale, IRB-approved, controlled clinical trial.
From a review of 30 patients with Long Covid (average 15 months) who completed the PVRP at 90 days, there was a 40% improvement in scores on the Post Covid Function Scale.
Though the group has accomplished much in the last two years, Hofmann stressed that the PVRP is still in an early stage, and the discovery process is ongoing. The program and the protocols continue to be evaluated and refined.
“Right now, we’re still in this phase of trying to understand what continues to be an emerging cluster of more than 200 different symptoms, and how to approach them from a systems medicine perspective. It’s a very complicated constellation and, it’s still very new. There are no proven therapies, no standards of care, and no clinical outcomes data from the NIH RECOVER initative,” she told Holistic Primary Care.
“There’s a window of opportunity now to demonstrate the effectiveness of this approach. At the same time, I feel very cautious about touting that we have something too soon. We need to continue enrolling patients in the program and the registry to track outcomes.
END


