




Administrative waste—defined as unnecessary non-clinical expenses that have no beneficial impact on patient care—accounts for roughly 15% of all US healthcare spending, according to a new analysis by the policy journal, Health Affairs.
Up to one-third of all money spent on healthcare in the US goes toward non-medical administrative costs. That’s nearly twice the level seen in other industrialized countries.
The Council on Health Care Spending and Value—a non-partisan consortium of economists and health policy experts—estimates that fully half of that can be classified as “wasteful spending,” defined as expenditure that “does not contribute to health outcomes in any discernible way.”
Basically, useless bureaucratic nonsense cost the nation between $285 billion and $570 billion in 2019, the year from which the Health Affairs authors based their estimates. The report attributes the waste largely to the “complexity and fragmentation of the US health care system.”

Not all administrative spending is wasteful. There’s a certain amount of necessary non-medical overhead intrinsic to the running of even the most efficient and patient-focused healthcare system. Administrative overhead typically includes billing-related costs such as claims management, clinical documentation, coding, and prior authorization procedures, as well as general overhead like marketing, credentialing, quality assurance, taxes, and of course, profits.
Depending on what is and isn’t included under the broad category of “administrative costs,” published studies put the percentage of total health dollars spent on administration in the range of 15% to 30%. Some studies only include billing-related costs, while others include non-billing overhead costs as well.
If healthcare represents 20% of the nation’s $23 trillion GDP, and 30% of healthcare dollars go to administrative costs, that means roughly 6.6% of the country’s total economic production goes to healthcare bureaucracy. And if half of that is wasteful, it means we’re now losing somewhere over $600 billion on pointless red tape.
But even at the low end of that range, administrative costs in the US are still double the amount spent on actual medical care for cardiovascular disease, and thrice what is spent for cancer care, say the Health Affairs authors.
20% of GDP
According to the Centers for Medicare and Medicaid Services (CMS), healthcare represented just 6.9% of the nation’s total gross domestic product (GDP) in 1970, roughly comparable to the amount spent in other industrialized nations.
By 2019, healthcare gobbled 17.7% of the US GDP. In the wake of Covid, the number hit 19.7%. In other words, healthcare now accounts for roughly one-fifth of the nation’s GDP. And it reached that point eight years earlier than CMS analysts had predicted, based on pre-pandemic growth trends.
The medical systems have pushed their most vital employees—physicians, nurses, and other practitioners—to the breaking point, and they deliver lower than expected outcomes on many health indicators. Yet, health insurance company stock prices have soared, and the people who run insurance companies continue to reward themselves handsomely.
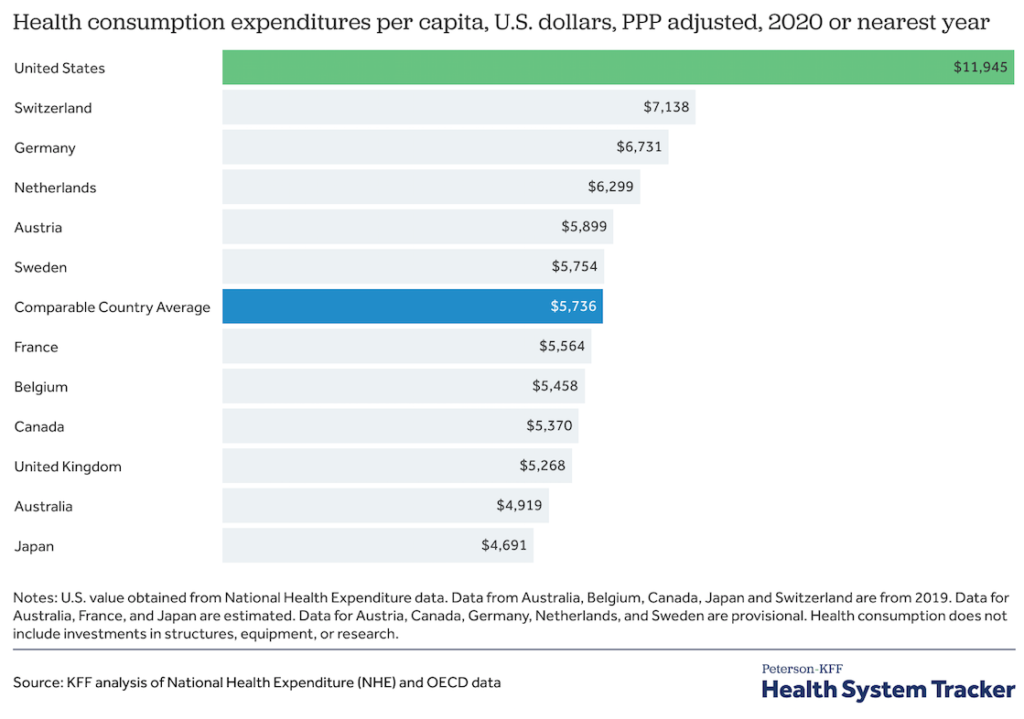
Healthcare spending is up all over the globe, but not nearly to the extent it has risen in the US. In 2020, healthcare expenditures were only 12.8% of GDP in the UK, the nation in second place behind the US on medical spending (Peterson-KFF Health System Tracker).
No doubt, some of the increase in healthcare spending reflects the emergence of new treatment modalities, and advances in diagnostic and therapeutic technologies. But a big chunk of it is administrative. And in that department, the US leads the world—by a wide margin.
According to a Peterson Foundation study using 2021 data from the Organization for Economic Cooperation and Development (OECD), the US spent $1,055 per capita on healthcare administrative costs. Germany, the country with the next highest administrative burden, spent $306 per capita—a more than three-fold difference.
According to a 2022 survey of nearly 600 physicians by management consultants Bain & Company, one in four physicians is considering a career switch outside of medicine. Nearly 90% of those who want to leave healthcare cite “burnout” as the main reason.
US healthcare clinics employ 44% more administrative workers than their Canadian counterparts. And US doctors and other clinicians devote far more of their working time to administrative duties than their colleagues to the north (13% versus 8%).
Doing some rough math, if healthcare represents 20% of the nation’s $23 trillion GDP, and 30% of healthcare dollars go to administrative costs, that means roughly 6.6% of the country’s total economic production goes to healthcare bureaucracy. And if half of that is wasteful, it means we’re now losing 3% of our GDP—somewhere over $600 billion—on pointless red tape.
Lack of Standardized Rates
To make their analysis, the Health Affairs panel the authors drew on a wide range of data sources including government health spending data, physician surveys, employment data, and cost analyses provided by health plans.
They attribute much of the wasteful spending to a lack of standardized fees and rates, especially for hospital services, and the lack of a common, centralized clearinghouse for submission and processing of electronic claims submissions.
US healthcare clinics employ 44% more administrative workers than their Canadian counterparts. And US doctors and other clinicians devote far more of their working time to administrative duties than their colleagues to the north.
They make an economic case for establishment of uniform all-payer rate schedules, which would reduce the administrative burden on practitioners, employers, and commercial insurers. But they acknowledge that politically this is unlikely to be embraced, as it is a central tenet of single-payer systems which are anathema to many policymakers in Washington.
Standardization of claims, and creation of a centralized clearinghouse—as exists in the banking industry to securely manage billions of transactions from a wide range of financial institutions—might be more feasible.
A central clearinghouse, “would receive batches of claims from multiple payers and providers and route them to the correct counterparty for each payment. The clearinghouse would also operate as a fraud detector to ensure that claims submitted were legitimate. Finally, it would confirm that the submitted information was compliant with privacy and security standards.”
David Cutler, a healthcare economist at Harvard, estimates that establishment of such a clearinghouse could save roughly $300 million annually in more efficient and accurate claims processing.
Prior Authorization Burdens
Prior authorization requirements represent another area of egregious waste, to say nothing of the burden they put on practitioners.
According to a 2019 American Medical Association survey, the typical US physician does an average of 31 prior authorizations per week, which sucks up nearly 15 hours of physician and staff time. More than one-third of practices have had to hire staff members to work full-time on this burdensome task. Nine out of 10 physician respondents said prior authorization requirements have a negative effect on clinical outcomes.
An analysis by the Council for Affordable Quality Healthcare, a non-profit consortium of health plans and medical industry stakeholders, shows that manual processing of prior authorizations costs roughly $13.40 per transaction, whereas processing via web portals costs just $7.19.
CAQH estimates that a widespread switch to completely digital prior authorization systems would save $417 million yearly. Alignment and harmonization of prior authorization criteria across health plans would further reduce wasteful spending.
Physicians spent an average of 785 hours per year—that’s nearly 33 days—on quality metrics reporting, and this cost approximately $15 billion per year.
Some argue that optimization of the prior authorizations process is simply putting lipstick on a pig. Rather, it would make more sense—and save more money—to minimize the demand for prior authorizations. The reality is that 90% of prior approvals sought by physicians from insurance plans are greenlighted, but not before putting everyone involved through a lot of costly, time-consuming rigmarole.
Harvard’s David Cutler proposes reducing or eliminating prior authorization requirements for the treatment of established chronic diseases and exempting practitioners with a documented history of appropriate care. Others advocate for a “gold card” type of system that exempts practitioners with demonstrated histories of appropriate care from prior authorization rules.
Quality control programs also cause a lot of wasted time and money, according to the Health Affairs team. There are more than 2,200 quality metrics used across the Medicare and Medicaid programs alone, and that’s in addition to the myriad metrics lists required by private payers, state, and local agencies. There is a glaring lack of standardization for quality assurance programs, and this is costly.
According to a 2016 study, physicians spent an average of 785 hours per year—that’s nearly 33 days—on quality metrics reporting, and this cost approximately $15 billion per year.
Doctors Want Out
Beyond the staggering economic costs, unnecessary administrative tasks are a major contributor to the practitioner burnout crisis. According to a 2022 survey of nearly 600 physicians by management consultants Bain & Company, one in four physicians is considering a career switch outside of medicine. Nearly 90% of those who want to leave healthcare cite “burnout” as the main reason.
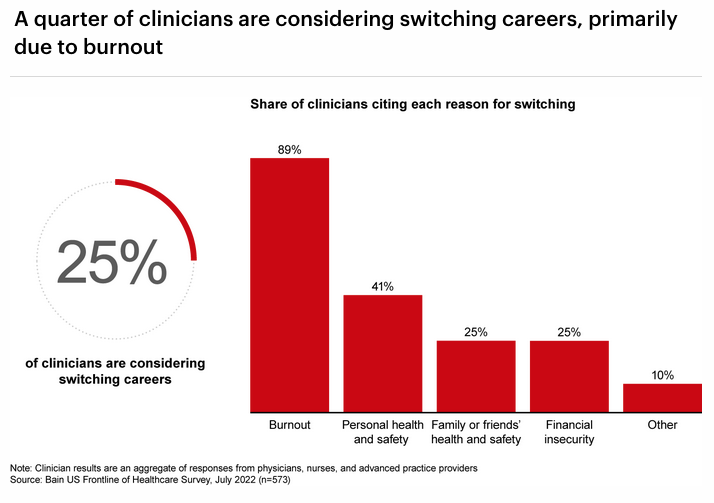
Clinician turnover rates have reached unprecedented levels, which has healthcare administrators worried. The Bain authors note that “potential resignation of a quarter of the workforce would further exacerbate the tight labor market, which is already on track to be short 38,000 to 124,000 physicians by 2034.”
There’s no doubt that duplicative and unnecessary administrative tasks are burdensome and costly. Health Affairs is right to call out the problem. But their analysis overlooks another factor that drives up costs while adding nothing to quality of care: corporate greed.
CEOs Sit Pretty
Though insurance industry CEO compensation dropped by 4% from 2020 to 2021, the heads of the six largest insurance companies averaged $19 million in total compensation last year, according to a 2022 report by Fierce Healthcare. Michael Neidorff, CEO for Centene, who died last April, topped the list, taking home $20,637,990 in salary, stock awards, stock options, and bonuses in 2021.
Karen Lynch, the CEO of CVS Health was number 2 on the list, with a total compensation package of $20,388,412—that’s 458 times the salary of the lowest paid CVS employees.
As the Health Affairs report clearly shows, healthcare as an industry is grossly wasteful. The medical systems have pushed their most vital employees—physicians, nurses, and other practitioners—to the breaking point, and they deliver lower than expected outcomes on many important indicators of public health.
And yet, insurance company stock prices have soared, and the people who run the insurance companies continue to reward themselves handsomely. They have little incentive to change the status quo. That’s not likely to cbe fixed by tweaking the billing systems or the requirements for prior authorization.
END


