




Clashes over vaccine mandates are the latest rifts defining a deeply politicized pandemic culture. In some states, local vaccination rules directly contradict national public health directives, putting hospitals and clinics in the difficult position of determining how to best safeguard patients and staff, amid a shifting landscape of conflicting directives.
I am watching one such vaccine mandate war unfold from my adopted home in rural Montana.
Here, a new state law makes it illegal for employers—including hospitals and medical clinics–to discriminate against workers on the basis of vaccination status. That rule conflicts with the Biden administration’s recently upheld federal vaccine requirement for healthcare workers, putting the burden on hospital administrators to determine which law they’re going to follow.
Direct Conflict
In May 2021, Montana became the first state to introduce legislation banning vaccine mandates for workers. Gov. Greg Gianforte (R) signed House Bill (HB) 702, just months after he assumed office. Codified under Montana’s Human Rights Act, the bill defines employee vaccine requirements as “discrimination.” It prohibits businesses from imposing vaccine rules on workers and claims to safeguard patients’ “personal and sensitive [healthcare] information” and medical record privacy.
By Fall, the Department of Health and Human Services (HHS) issued a COVID-19 vaccine mandate for nearly all workers at facilities that receive federal funds through the Centers for Medicare & Medicaid Services (CMS). That rule includes hospitals, nursing homes, and other health clinics.
Eschewing the CMS vaccine rule could result in major revenue shortfalls if CMS enforces the mandate. That could lead to hospital and clinic closures and, “drastically reduce access to healthcare services for Montanans .
Several health systems throughout Montana promptly announced their intention to comply with the new federal regs. But that puts these networks in direct conflict with Gov. Gianforte and the state’s new law.

Surging Caseloads
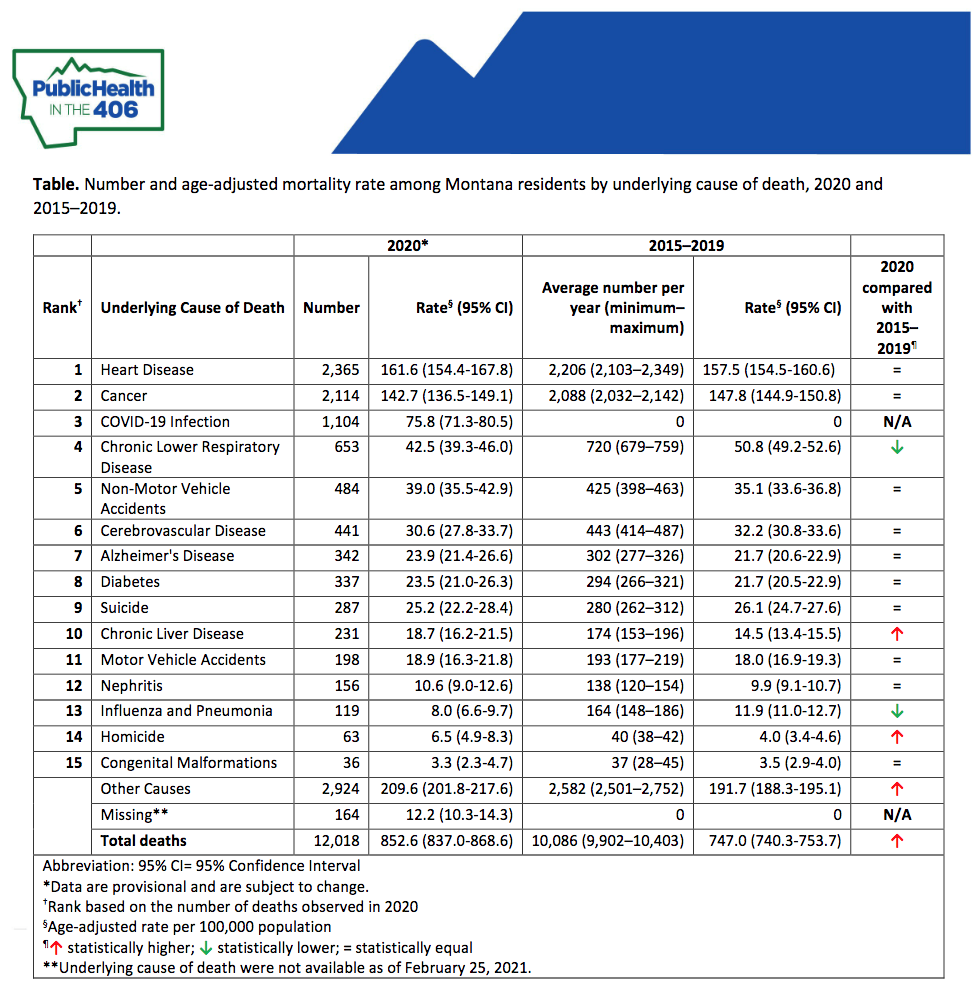
Montana has one of the lowest vaccination rates in the country: 54% of the state’s population of just over 1 million are fully vaccinated as of mid-January. Roughly 3,000 Montanans have died from COVID-19, the third leading cause of death in the state in 2020.
Though prevalence and mortality are relatively low compared to more populous and urban states, the pandemic is taking a severe toll on some Montana communities. The state is home to one of the country’s largest Native American populations, and COVID was the top cause of death in Montana’s native communities in 2020. All-cause mortality among American Indian Montana residents increased by 36% that same year, compared with the previous five years.
Last October, when COVID hospitalizations surged, some Montana facilities had to implement crisis of care standards and care-rationing protocols. Hospitalizations are once again rising sharply across the state as Omicron spreads.
A Threat to Access
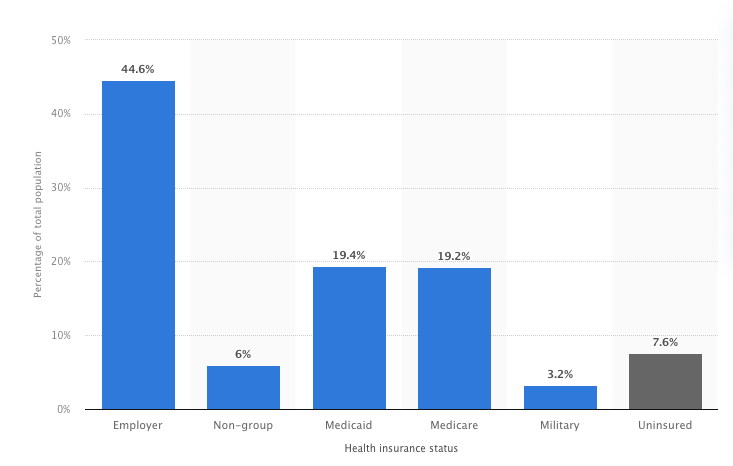
More than a half a million Montanans receive coverage through Medicare and Medicaid. Data released late last year indicate that nearly 40% of the state’s population relied on the federal programs in 2020.
“Payments received from Medicare and Medicaid help support services available to all of us,” said MHA president and CEO Rich Rasmussen in a recent statement. CMS funding represents 70% of all revenue at Montana hospitals, and is “critical to the financial viability and continued operations” of medical centers statewide.
According to the Montana Hospital Association (MHA), eschewing the CMS vaccine rule could result in major revenue shortfalls if CMS enforces the mandate. That could lead to hospital and clinic closures and, “drastically reduce access to healthcare services for Montanans over 65 years of age, working and low-income families, pregnant women and children, and people with disabilities.”
In other words, elderly and high-risk individuals who already have limited access to healthcare, would have their access further compromised.
With the Supreme Court’s split decisions—supporting CMS but dashing OSHA–it’s now up to individual employers to determine how the final rules impact their businesses.
The Court did not explicitly address the question of how, on a practical level, federal rules apply in places like Montana, with conflicting state-level laws.
“Failure to comply (with the CMS mandate) means that CMS could terminate our participation in the program, which will threaten our ability to care for those in our services,” reported Logan Health, a hospital system based in northwestern Montana.
In November, Logan announced that its more than 4,000 employees must be fully vaccinated for COVID by early December in order to continue working onsite. The original CMS deadline for employee vaccinations was January 4.
But in courts around the country, officials wasted no time challenging federal mandates. Louisiana and Missouri each filed separate actions questioning the legality of the CMS requirement. District court judges issued preliminary injunctions against the rule’s enforcement in November, temporarily pausing the vaccine requirements for healthcare staff.
Keeping Up with the Judges
Those decisions forced medical centers to suddenly reverse course. Logan Health suspended its staff vaccination plan merely a week after rolling it out.
On January 13, the Supreme Court issued a final ruling formally upholding the CMS regulation. It concluded that the Secretary of HHS acted within his authority when he determined that “a vaccine mandate was “necessary to promote and protect patient health and safety.”
“Healthcare facilities that wish to participate in Medicare and Medicaid have always been obligated to satisfy a host of conditions that address the safe and effective provision of healthcare,” the assenting justices wrote. That includes long-standing rules specifically addressing infectious disease prevention, control, and surveillance within medical settings––regulations created well before the threat of COVID-19.
The justices also point out that staff vaccine policies to prevent other diseases are standard practice. “Vaccination requirements are a common feature of the provision of healthcare in America,” they write. Healthcare facilities nationwide already require shots against measles, mumps, and rubella, hepatitis B, and influenza as a condition of employment.

In a press release shortly after the Supreme Court ruling, MHA’s Rasmussen noted that, “With the CMS COVID-19 vaccine requirement once again in place for healthcare facilities, Montana hospitals will adjust their policies to ensure compliance with the federal law. CMS has asserted this federal requirement takes priority over state and local law.”
Hospitals around Montana are once again requiring workers to get the shots. Logan Health announced on Jan. 19 that all staff must be fully vaccinated by February 15.
But even if Montana’s medical facilities do comply with CMS’s requirements, other business sectors will abide by the state’s mandate prohibition.
Without strong federal vaccine standards for workers outside of healthcare, public health policy here and in other states will be governed by a patchwork of regional laws and executive orders. And these policies vary significantly from state to state.
A Political Battle
Mandates do raise overall vaccination rates. Data from a White House report on vaccine strategies show increased uptake in the vast majority of communities that have implemented requirements.
The justices point out that staff vaccine policies to prevent other diseases are standard practice. Vaccination requirements are a common feature of the provision of healthcare in America. Healthcare facilities already require shots against measles, mumps, and rubella, hepatitis B, and influenza as a condition of employment.
A recent Axios/Ipsos poll suggests that “the majority of employed Americans support vaccine and mask mandates in their workplace.” But while 60% support their employers’ vaccine requirements, only 14% are supportive of firing colleagues who do not comply.
Even as the Omicron wave engulfs health centers around the country, opposition to vaccine mandates remains strikingly high, especially in Republican-governed states. For some, the rapid spread of Omicron–even among fully vaccinated people–is evidence that the shots are ineffective, and therefore, unnecessary.
Twenty states––all with Republican governors––currently prohibit businesses or government agencies from requiring people to prove that they’re vaccinated. Some governors are using emergency orders to halt “proof-of-vaccination” requirements for entry into restaurants, community events, and public activities. Others, including Montana, ban vaccine rules or “immunity passports” via permanent legislation.
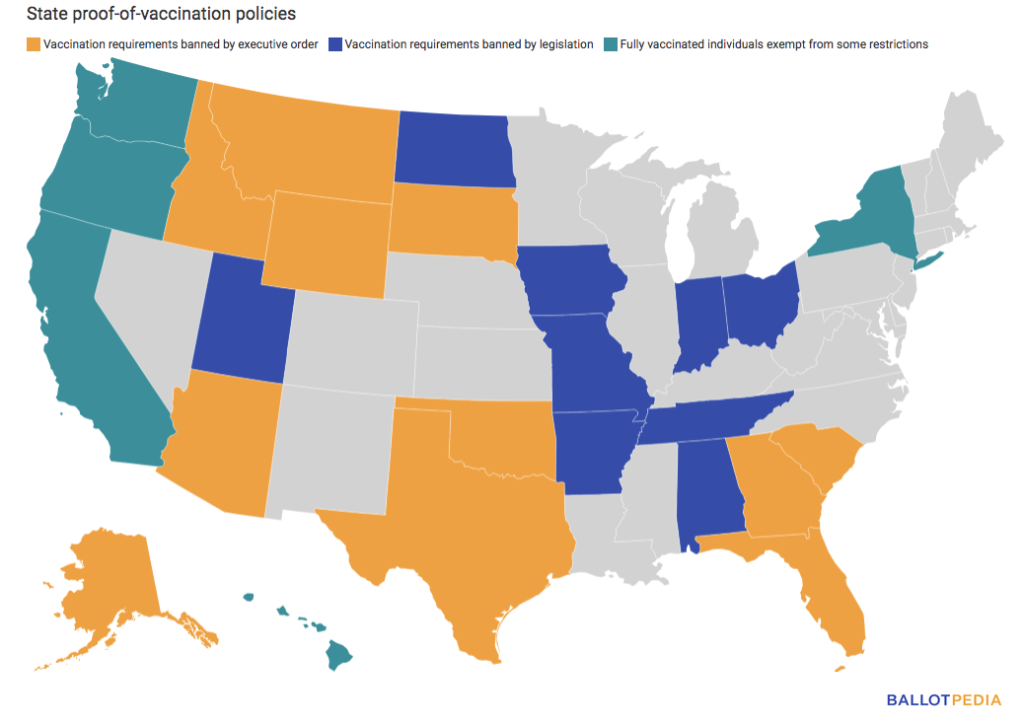
State laws in Florida ban employer vaccine mandates, prohibit school face mask policies, and impose fines of up to $50,000 per worker on businesses that violate the state’s anti-mandate rules, which—in true Orwellian fashion–are described as “employee health protections.”
The scene is markedly different in Democrat-led states. California, New York, Hawaii, Oregon, and Washington permit businesses to prohibit entry of unvaccinated people and allow individuals with proof-of-vaccination to bypass restrictions that apply to non-vaccinated people.
Eighteen states are taking a more hands-off approach, neither outlawing nor establishing vaccine requirements.
To Treat or Prevent?
The Biden administration pushed for a nationwide vaccination-or-test policy for businesses employing 100 or more individuals, via the Occupational Safety and Health Administration (OSHA). The Supreme Court’s second January 13 ruling struck it down.
Opponents of the OSHA mandate––private businesses and Republican-led states––accused the agency of overreach, claiming that authority to issue emergency public health rules falls under the purview of state and local governments only. Many also argued that the decision to take a vaccine should be a personal choice, not a requirement as a condition of employment.
With the Supreme Court’s split decisions—supporting CMS but dashing OSHA–it’s now up to employers to determine how the final rules impact their businesses.
Rather than tightening prevention efforts, including vaccines, some politicians and business leaders are instead promoting a wait-and-treat approach. Their message, in essence, is take no precautions and wait until you catch COVID to do anything about it.
That’s based in the logic that only a small percentage of infected people will develop severe or fatal symptoms, and that effective therapies are on the horizon.
There are indeed several promising new antiviral drugs that could change the course of the pandemic moving forward. While they will undoubtedly help save lives, the myopic focus on treatment overlooks the countless additional lives that could be spared through more intensive prevention efforts.
Advocates of wait-and treat are also willing to ignore the overwhelming pressure that ill and unvaccinated COVID patients place on healthcare systems and practitioners. And they fail to acknowledge the staggering number of patients who develop long COVID.
Few Walk-Outs
A prevailing argument against jobsite vaccine rules is that many employees will quit their jobs, or choose to be fired, rather than get vaccinated.
This is an oft-expressed fear in my community, where staffing gaps are a real and chronic concern. Many of Montana’s rural counties are officially recognized as health professional shortage areas. Severe staffing inadequacies and limited access to services are perennial problems. COVID simply exacerbated existing issues in rural healthcare delivery.
Do healthcare personnel really walk out in opposition to vaccine mandates? Sure, some do so, but not in large numbers.
So far, healthcare systems with vaccine requirements are seeing only minimal staff loss. Fierce Healthcare recently published data from 59 hospitals and healthcare networks across the country that have implemented mandates: none report attrition rates of more than 1% of total workforce due to vaccine-related resignations or terminations.
Do healthcare personnel really walk out in opposition to vaccine mandates? Sure, some do so, but not in large numbers. Healthcare systems with vaccine requirements are seeing only minimal staff loss.
A 1% workforce loss is not nothing, especially in facilities already short-staffed. But neither is it the apocalypse that mandate critics predicted. That 1% walkout rate needs to be weighed against the number of medical professionals temporarily or permanently sidelined by COVID itself.
“A Menace in Work Settings”
Unsurprisingly, some of the country’s most prominent medical organizations and experts support the OSHA vaccine requirement. The American Medical Association, American College of Physicians, National League for Nursing, American Public Health Association, and many others signed a joint statement expressing their collective backing of a broad federal mandate. Several also filed an amicus brief opposing legislative efforts to obstruct the requirement.
In a January 13 press release, Secretary of Labor Marty Walsh defended the OSHA vaccine-or-test policy, noting that OSHA’s current guidance basically just outlines the CDC’s recommendations.
The Occupational Safety and Health Act of 1970 grant OSHA the power to enact temporary emergency standards if “employees are exposed to grave danger from exposure to substances or agents determined to be toxic or physically harmful or from new hazards” and if such emergency standards are deemed “necessary to protect employees from such danger.”
According to the judges who backed OSHA’s vaccine rule, COVID clearly “poses grave dangers.”
“The disease has by now killed almost 1 million Americans and hospitalized almost 4 million,” they write. “It spreads by person-to-person contact in confined indoor spaces, so causes harm in nearly all workplace environments…COVID–19, in short, is a menace in work settings.”
With the Supreme Court’s split decisions—supporting CMS but dashing OSHA–it’s now up to employers to determine how the final rules impact their businesses.
The Court did not explicitly address the question of how, on a practical level, federal rules apply in places like Montana, with conflicting state-level laws.
Here, it remains technically impossible for clinics to comply with both federal and state law. Administrators and healthcare workers in our state remain in an untenable position. Gov. Gianforte has not yet issued a formal response to the CMS over-ride of his anti-mandate law.
With further legal actions surely still to come, a fundamental question remains unanswered: whose health deserves to be protected during a public health emergency?
END


