



Back in March of 1918, the ‘Spanish flu’ was spreading rapidly across the globe, killing millions and terrifying a world already ravaged by the first world war. During that summer the pandemic died down, only to rear its ugly head the following winter, killing many more.
More than a century later, we are now into the third winter of the COVID-19 pandemic. By now, we should know what to expect: a surge of COVID cases, compounded by a spike in influenza as well.
The winter of 2020-21 was unique in that flu prevalence was far lower than historical norms. Some suggest that this was due to a misallocation of flu symptoms to SARS-CoV-2. Others credit physical distancing, masking, and curtailment of travel as people tried to protect themselves from COVID.
This year, it’s a different story. People have been traveling, gathering, attending mass events. Many have been far less fastidious about masking than they were in the early months of 2020.
Where to Start?
What can we do? How do we help our patients protect themselves and their families from the twin threats of COVID and flu?
We all know that primary recommendations always begin with lifestyle choices and food selections. That’s obvious. And we also know about Vitamin A, Vitamin C, Vitamin D, Zinc, Curcumin, Quercetin, NAC…there’s a long list of nutrients and herbs that can support strong immune system defenses.
I strongly recommend the Institute for Functional Medicine’s excellent compilation of information on nutrients with good scientific backing for potential prevention of COVID (and other viral illnesses). Their review includes dosages, and purported mechanisms of action. But the IFM documents don’t give any priority as to where to begin. That judgment is, rightfully, left up to individual clinicians
Given the real-world challenges of working with patients in brief episodic visits, where should we begin? What is the top priority for the majority of patients?
I believe there is one option that stands above all the others, and that should be the initial highest priority—the intervention that will give the biggest “bang for your buck.” It is Vitamin D.
There are many reasons why ensuring robust Vitamin D levels is the most potentially impactful intervention on that checklist. Reducing the impact of COVID is a big one.
Putting it simply, mortality from COVID-19 appears to be much, much lower if your serum Vitamin D is between 50-80ng/ml (125-200nmol/L).
That was the conclusion of a recent metanalysis of Vitamin D studies published in the journal Nutrients in October. The title of this paper really says it all: ‘‘COVID-19 Mortality Risk Correlates Inversely with Vitamin D3 Status, and a Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3.”
Drawing on data from one population study and seven hospital-based studies, the authors conclude there is “strong evidence that low D3 is a predictor rather than just a side effect of the infection.”
They note that, “At a threshold level of 30 ng/mL (75nmol/L), mortality decreases considerably. In addition, our analysis shows that the correlation for the combined datasets intersects the axis at approximately 50 ng/mL (125nmol/L), which suggests that this vitamin D3 blood level may prevent any excess mortality.”
Unfortunately, most Americans are not even close to that range.
Raise D, Reduce Mortality
Borsche and colleagues contend that raising mean Vitamin D levels to that 50 ng/mL mark could reduce COVID mortality to near zero, regardless of vaccine status—at least in theory.
They paint an optimistic picture: “From a medical point of view, this will not only save many lives but also increase the success of vaccination. From a social and political point of view, it will lower the need for further contact restrictions and lockdowns. From an economical point of view, it will save billions of dollars worldwide, as vitamin D3 is inexpensive and—together with vaccines—provides a good opportunity to get the spread of SARS-CoV-2 under control.”
These are bold claims, and we need to keep in mind all the caveats we would apply to any systematic review: concern for study selection bias; statistical manipulation of heterogenous data sets; failure to control for all potentially confounding variables.
But with all those caveats, what’s the danger of testing a patient’s Vitamin D level? What’s the cost/benefit ratio for supplementing to get the level up over that 50ng/mL level? The danger is zero. The cost is minimal. And the benefit? Potentially saving someone’s life.
The authors acknowledge that “empirical data on COVID-19 mortality for vitamin D3 blood levels above 35 ng/mL are sparse,” and that the medical community will need definitive large-scale randomized controlled trials in order to justify Vitamin D supplementation as a public health measure.
Still, from a practical patient care perspective, testing for Vitamin D and supplementing to raise levels in people who are deficient seems like a no-brainer. It’s a simple, inexpensive test—there’s even a finger-prick blood spot version with high sensitivity and specificity that we have used for years.
An Epigenetic Regulator
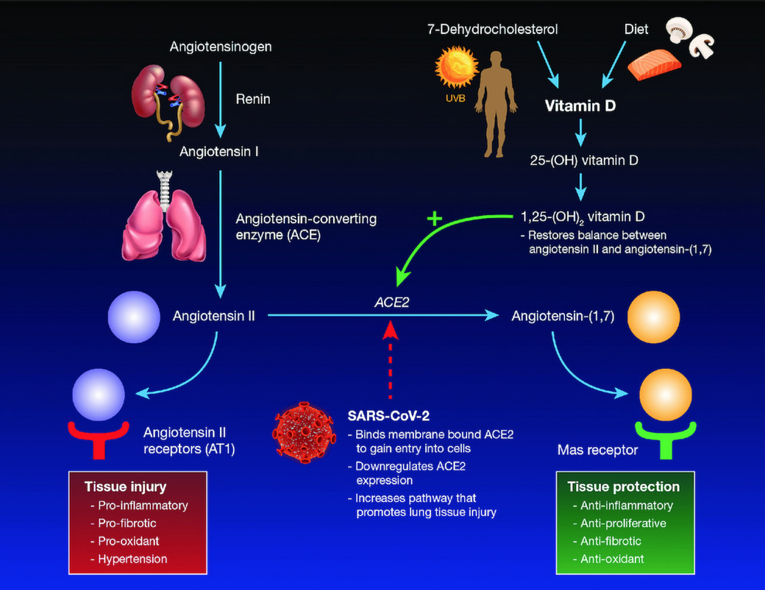
We know that Vitamin D is a powerful epigenetic regulator influencing more than 2,500 genes including many that affect the immune system.
Vitamin D enhances cellular innate immunity partly through the induction of antimicrobial peptides, including human cathelicidin LL-37 and defensins. We learned from Herr and colleagues almost 15 years ago that cathelicidins exhibit direct antimicrobial activities against a spectrum of microbes, including Gram-positive and Gram negative bacteria, enveloped and non-enveloped viruses, and fungi
Borsche and colleagues hypothesize that raising serum 25(OH)D levels to above 50 ng/mL might actually mitigate the impact of outbreaks caused by variants that are not susceptible to current vaccines.
The epidemiological data suggest that after rickets, COVID-19 represents the second historical association of Vitamin D deficiency and life-threatening disease in humans. Though we do not yet have definitive data showing that supplementation can reverse COVID the way it can reverse rickets, the strength of this correlation—which has been observed in populations all over the world—warrants our medical attention.
What to do when someone’s Vitamin D level is low? What’s the best way to supplement?
There is a lot of confusing information out there. Much of that confusion arises because the Institute of Medicine’s Dietary Reference Intakes (800 mg per day for Women 19 to 50 years; 1,000 mg for women over 50; 800 mg for men up to 71, and 1,000 for men over 71) are based on the century-old dose ranges used to prevent Rickets.
Vitamin D science has improved vastly over the last 100 years. We now know so much more.
Quelling the Cytokine Storm
Consider the recent paper by Lakkireddy and colleagues, which showed startling positive results using targeted daily supplementation in the dose range of 60,000 IUs of vitamin D for 8 or 10 days (depending upon subjects’ BMI) in a cohort of hospitalized COVID-19 patients. All underwent standard conventional therapies for COVID prior to randomization to the Vitamin D or no Vitamin D arms.
The study showed:
- Vitamin D levels increased from 16 ± 6 ng/ml to 89 ± 32 ng/ml among 44 subjects recieving “Pulse D therapy” (60,000 IUs of Vitamin D in the form of aqueol nano solution (Deksel) per day for 8 days for subjects with body mass index (BMI) of 18–25, and for 10 days for subjects with BMI > 25).
- Compared with those not receiving Vitamin D, those in the Pulse D group showed highly significant (p < 0.01) reductions of all the measured inflammatory markers (C-reactive protein, lactate dehydrogenase, interleukin-6, ferritin, neutrophil/lymphocyte ratio).
Elevation of Vitamin D levels into the mean range of 80–100 ng/ml has significantly reduced the inflammation associated with COVID-19, just 11 days after the start of high-dose supplementation—and without any side effects.
Basically, we’ve got a therapy here that can reduce all the markers of the COVID “cytokine storm,” with no side-effects. What more could we ask for? I am certain that if these results were from a pharmaceutical study, they would be a lead story in every news broadcast worldwide.
I urge you to take the time and read the Lakkireddy paper, and the Borsche metanalysis. With a very simple test and a relatively inexpensive nutraceutical intervention, we have the potential to greatly reduce our patients’ risk of severe illness, and to reduce mortality this winter.
My recommendation is that we all make sure every patient is aware of his/her vitamin D levels, and to work with all our patients to get those levels up between 50-80ng/ml. If they are exposed to SARS-CoV-2 their risk of severe illness could be greatly reduced. This easily accessible intervention could save lives. You may even want to download the Borsche and Lakkireddy articles to share with patients, to underscore the importance of keeping Vitamin D levels up.
If that evidence is not enough to convince you, then take a look at the 2020 study by Michael Holick and his group at Boston University working in conjunction with Quest Diagnostics. They looked at SARS-CoV-2 seropositivity rates and vitamin D levels in data from more than 190,000 subjects from all 50 states, tested between March and June of 2020.
Overall, the SARS-CoV-2 positivity rate was 9.3%, and the mean seasonally adjusted 25(OH)D was 31.7, across the entire cohort.
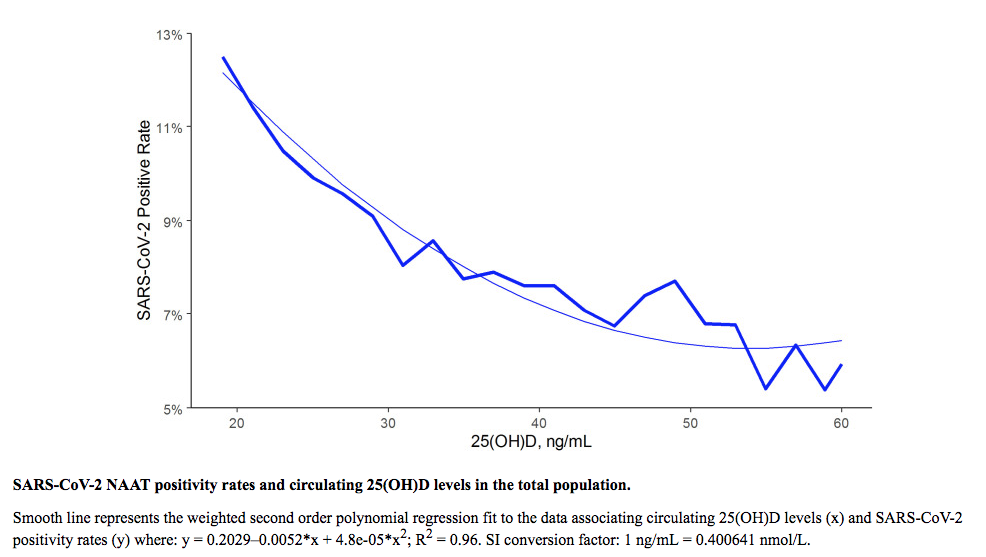
The seropositivity among those with Vitamin D deficiency—defined as 25(OH)D levels under 20ng/mL) was significantly higher at 12.5%, compared to 8.1% in those with “adequate” levels (30-34 ng/mL), and 5.9% in those with levels of 55ng/mL or higher.
For each 2.5nmol/L (1 ng/mL) increase in circulating 25(OH)D, there was an associated 1.6% decreased risk of seasonal infection. This association persisted across latitudes, races/ethnicities, and genders.
Those findings are consistent with a study published ten years ago in the British Journal of Nutrition, looking at the relationship of Vitamin D status and seasonal respiratory infections. After adjusting for adiposity, lifestyle, and socioeconomic factors, the investigators found that for each 10 nmol/L (4ng/mL) increase in 25(OH)D, there was an associated 7% lower risk of respiratory infections.
Cardiovascular Benefits
Beyond concerns about COVID or influenza, there are many other reasons to keep vitamin D levels up.
Consider the brand new study from researchers at the Australian Center for Precision Health, showing that Vitamin D deficiency is associated with marked increases in the risk of hypertension and cardiovascular disease.
The Australian team, headed by Elina Hypponen, PhD, MPH, evaluated U.K. Biobank data on 44,519 patients with CVD, and 251, 269 case controls. They considered a serum 25(OH)D level of less than 30 nmol/L to be deficient, levels in the 30-50 nmol/L range to be mildly deficient, and levels over 50 nmol/L to be sufficient.
Across this massive cohort, the average serum 25(OH)D concentration was 50 nmol/L (20ng/mL), but 55% of participants had low levels, and 13% had severe vitamin D deficiency, with levels below 25 nmol/L (10ng/mL)
Here’s the take-home point: the people with serum 25(OH)D levels of 25 nmol/L had 11% higher odds of developing CVD compared with those whose levels were at the 50 nmol/L mark.
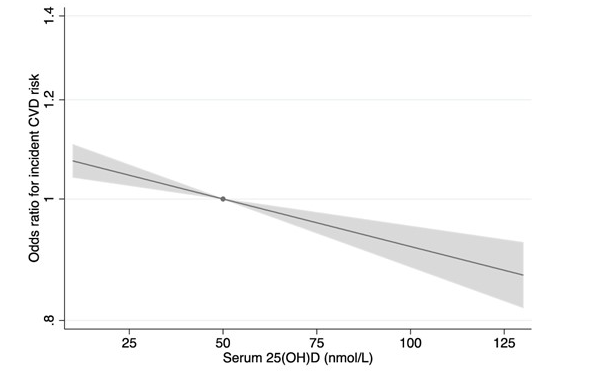
They saw a similar pattern for both systolic and diastolic blood pressure. Individuals with Vitamin D levels of 25 nmol/L had 0.7 mm Hg higher systolic BP and 0.25 mm Hg higher diastolic BP compared with those whose D levels were 50 nmol/L.
Every 10 nmol/L increase in Vitamin D level was associated with a 1.6% lower odds of developing heart disease. The authors estimate that 4.4% of all CVD cases could have been prevented by increasing vitamin D-deficient individuals to serum 25(OH)D levels of at least 50 nmol/L.
Given that CVD is still a top cause of death among all people worldwide, that’s an important finding.
All of the studies I’ve cited here, whether looking at COVID-19 and other respiratory infections or CVD, point to a similar message: incremental increases in serum Vitamin D levels in those who are low, produce incremental decreases in risk of disease.
If you’ve read this far, I think it’s safe to say that you have a strong interest in guiding patients toward living their healthiest possible lives, with as natural an approach as possible. In my opinion, the top priority action step we can take in helping patients protect themselves this winter is to test their Vitamin D levels.
If they’re low, we can give them the relief of knowing that within a couple of weeks, at very low cost and little risk of adverse effects, they can get those levels up to the point where they will greatly reduce their risk of respiratory infections and cardiovascular disease, and improve their overall health.
END
Tom O’Bryan, DC, DACBN, CIFM is an internationally recognized and sought-after speaker and workshop leader specializing in wheat-related disorders, their impact on health, and the development of autoimmune diseases as they occur inside and outside of the intestines. He holds teaching faculty positions with The Institute for Functional Medicine and the National University of Health Sciences. He has trained and certified tens of thousands of practitioners around the world in advanced understanding of the impact of wheat sensitivity and the development of individual autoimmune diseases. Dr. O’Bryan is founder of TheDr.com and the visionary behind The Gluten Summit: A Grain of Truth, and Betrayal: The Autoimmune Disease Solution They’re Not Telling You. Learn more at TheGlutenSummit.com.


