For
many patients, the origins of autoimmunity aren’t just rooted in genetics or
environmental triggers. Latent infections and chronic stress can silently shape
immune responses for years before a formal diagnosis is made. And when left
unaddressed, these invisible drivers may sabotage even your best interventions.
Join
Dr. Corey Schuler for this free webinar, offering a clinically rich,
thought-provoking exploration that connects the dots between stealth pathogens,
the stress response, and immune system chaos.
This
webinar explores how latent infections and chronic stress contribute to
the development and progression of autoimmune diseases. Dr. Schuler will discuss
the physiological and clinical intersections between stress, infections, and immune
dysregulation, along with practical strategies to support patients with
autoimmunity.
The
session will also cover hormone dynamics, key lab assessments, foundational
treatment approaches, and a case study of a patient with Hashimoto’s
thyroiditis.
Understand the interplay between latent
infections and chronic stress in autoimmune pathogenesis
Identify biomarkers and diagnostic strategies
Integrate holistic treatment approaches
Enhance
patient-centered care for autoimmune disorders
SPONSORED BY ALLERGY RESEARCH GROUP
Corey Schuler, PhD, FNP, CNS has dedicated his career to advancing the science and clinical art of integrative medicine. He currently serves as director of medical affairs for Allergy Research Group. He is a family nurse practitioner and practices holistic primary care at Synergy Family Physicians in White Bear Lake, Minnesota.
The proliferation of fraudulent clinical research has reached epidemic proportions, creating a major headache for practitioners. There were roughly 10,000 fraudulent papers retracted by medical journals last year, the highest number on record. While the problem affects all areas of medicine, the field of nutrition is especially vulnerable (Image: PeopleImages–Yuri A/Shutterstock)
Good
medical practice is based on trust.
Patients trust that practitioners are knowledgeable, and that they use their knowledge intheir patients’ best interests. In turn, practitioners trust that researchers run their studies honestly, and that editors and peer-reviewers of the medical journals carefully scrutinize the papers they receive, sift out the garbage, and only publish studies that pass clinical, statistical, and ethical muster.
Research itself is also a trust proposition. From the lead investigators who design trials, and the Institutional Review Boards (IRBs) that approve them, to the research assistants and post-doctoral fellows who crunch the data, and the authors who write and submit the papers, there’s a thread of trust that depends on the right people doing the right things at each point along the path.
That’s
how it ought to be in an ideal world. But the hard truth is, this is not an
ideal world.
It’s
an open secret that medical research fraud is rampant.
A recent article
in The Guardian estimated that last year, there were more than 10,000 fraudulent
papers retracted by journals across the sciences. That’s the highest number of
retractions ever recorded. And this is likely just the surface layer of the
problem.
Epidemic
Proportions
Alan Gaby, MD, author of the textbook, Nutritional Medicine. Dr. Gaby has read and reviewed tens of thousands of nutrition papers over the years. “Several hundred papers per year….raise questions about whether the research is legitimate.”
Research fraud is widespread across all domains of science. As revealed in a Wall Street Journal article published on May 14, the proliferation of fraudulent papers prompted Wiley–one of the world’s oldest and most respected academic publishers –to shutter 19 of the journals under its recently acquired Hindawi imprint.
Wiley bought Hindawi, an Egyptian publisher of science journals in 2021, for $298 million. By May 2023, Wiley had to discontinue four titles–Computational and Mathematical Methods in Medicine, Journal of Healthcare Engineering, Journal of Environmental and Public Health, and Computational Intelligence and Neuroscience –because of the prevalence of bogus papers.
One year later, Wiley announced the discontinuation of 19 other titles, many though not all of which, are medical or healthcare-related. The company states that the closures reflect an effort to integrate Hindawi with Wiley’s existing journal portfolio, and to eliminate redundancies and journals that “no longer serve their communities.” But the Wall Street Journal claims that some of the journals on this list “were infected by large scale fraud.”
Over the past 2 years, Wiley has retraced more than 11,000 papers across journal holdings which represent hundreds of scientific disciplines. And Wiley is not alone. Other major academic publishers are also scrambling to deal with the rapid proliferation of fraudulent papers.
The problem of research fraud is especially prevalent in the field of nutrition, says Alan Gaby, MD, a holistic physician who is author of the massive textbook, Nutritional Medicine.
Now
in its third edition, Gaby’s book contains nearly 17,000 research citations and
covering the use of herbs and nutraceuticals for more than 400 specific health
conditions. Suffice to say, Dr. Gaby has probably read more clinical research
papers on nutrition than anyone on the planet.
He
contends that the problem of research fraud has reached epidemic proportions.
“Over
the past 50 years, I’ve probably reviewed about 50,000 papers. And about 15
years ago, I became aware of some irregularities in a lot of the research. A
growing number of papers left me wondering if the research had actually been
done at all, or if the data were simply fabricated.”
Fraudulent research corrodes public trust; it misleads clinicians; and it skews metanalyses. Once marketers and sales people get hold of it, they easily turn it into dishonest and misleading product claims. At minimum, ordinary people get ripped off. At the extreme, people could get hurt.
Gaby
says the number of suspicious—or at least highly questionable–papers has
surged dramatically in recent years, in part due to the growth of open access publishing and the proliferation of small, poorly refereed open-access
journals and websites, some of which are pay-for-play operations.
But
open-access is only part of the problem. Gaby says he’s seen numerous instances
in which dubious nutrition studies have appeared in venerable, “high impact”
(ie, widely-cited) conventional medical journals.
“Several
hundred papers per year, in my view, raise questions about whether the research
is legitimate.”
Gaby
stressed that it is difficult—and time consuming—to prove definitively that a published
paper is fraudulent. But there are an alarming number of studies that simply do
not hold up to careful scrutiny. When this happens in respected peer-reviewed
journals, as it sometimes does, it suggests that peer reviewers are failing to
do their jobs, or that they’re turning a blind eye to shoddy work.
Dr.
Gaby is not the only physician ringing alarm bells. Several years ago, a team
of researchers based in New Zealand called out two prominent Japanese
investigators—Yoshihiro Sato and Jun Iwamoto—claiming that nearly 300 of their
published papers in 78 medical journals, had major methodological flaws, ethical
lapses, and signs of fabrication.
Sato,
who died in 2017, and Iwamoto were both prominent professors at Japanese
universities. Their work was primarily focused on bone metabolism, and they
published many studies looking at the effects of Vitamin D, Vitamin K, and folate.
They also studied prescription drugs like methylprednisolone, hormone
replacement therapy, and valproic acid. Some of their research extended into
fields like neurology and gastroenterology.
Alison Avenell, PhD, University of Aberdeen, Scotland. Dr. Avenell headed an effort to expose one of the biggest legacies of research fraud in history
Studies
by Sato and Iwamoto have appeared in some of the world’s top journals,
including the Journal of theAmerican Medical Association (JAMA),Neurology, and the Journal of Bone and Mineral Metabolism.
The
saga began in 2006, when biochemist Alison Avenell, the Chair of Health Services Research at the University of
Aberdeen, Scotland, was delving into the question of whether vitamin D could
reduce bone fractures. While plumbing the literature, she came across two
studies by Sato. One involved a cohort of stroke patients, and the other, patients
with Parkinson’s.
Avenell
noticed that in both studies, the patient populations had exactly the
same mean body mass indexes. That, she thought, was statistically unlikely. She
started digging more deeply, and the more she looked, the more anomalies she
found: unreasonably large treatment effects, unusually large patient
populations, plagiarized text, numbers that simply didn’t add up.
“Expressions
of Concern”
Soon
after, Avenell teamed up with Andrew Grey, Mark Bolland, and Greg Gamble of the
University of Auckland, New Zealand. The team undertook an exhaustive review of
292 papers published by Sato alone or in partnership with Iwamoto.
In
2016, this intrepid team published an in-depth takedown of 33 studies by Sato,
Iwamoto, or both. They notified 78 journals that most, if not all, of the
nearly 300 papers published by these two researchers were flawed at best,
fraudulent at worst.
Not
long before he died, Yoshihiro Sato admitted that he falsified research, and
absolved Jun Iwamoto of any direct responsibility.
German anesthesiologist, Joachim Boldt, MD, formerly at the Klinikum Ludwigshaven, holds the global record for most papers retracted. A shocking 194 of Boldt’s published studies have been deemed fraudulent.
The
so-called “Sato Affair” is one of the biggest legacies of medical research
fraud in history. According to Retraction
Watch, a
website founded by former Medscape VP, Ivan Oransky and science writer Adam
Marcus, that monitors retractions across a vast range of scientific
disciplines, Sato and Iwamoto hold the 4th and 6th places
for highest number of papers retracted worldwide.
Who’s number one? That dubious honor belongs to Joachim Boldt, a German anesthesiologist and ICU physician, who’s had a stunning 194 of his published papers retracted because of data fabrication and lack of ethics board approval.
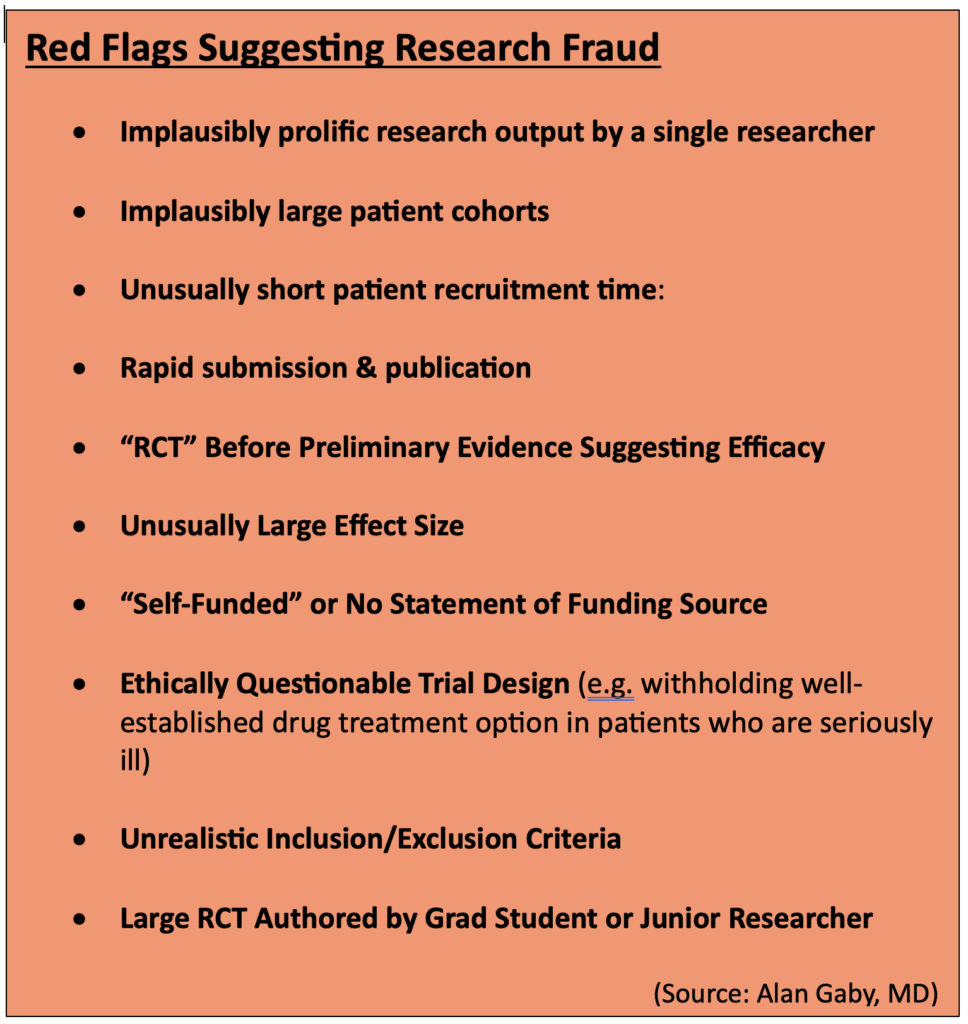
Red
Flags for Fraud Detection
With
fraudulent research on the rise across the medical landscape, and peer review
boards apparently faltering, practitioners need to sharpen their critical
thinking skills when reading clinical studies. But one need not become a
statistician.
“Several hundred papers per year, in my view, raise questions about whether the research is legitimate.”
–Alan Gaby, MD
Over
the years, Dr. Gaby has identified ten red-flag warning signs that raise the index
of suspicion about misconduct or outright fraud:
Implausibly prolific research output by a
single researcher: A good clinical researcher typically completes and publishes 3-4 large,
randomized, double-blind, controlled trials in a period of 5 or 10 years, Gaby
says. Yet, some researchers publish 10, 20, or even 30 papers in that time
span. “Whenever you see implausibly large research output, it makes you wonder
how could they have possibly done all of that research.”
Implausibly large patient cohorts: Gaby says
that over time, people who read a lot of studies develop a good sense of how
many people could be reasonably enrolled in a given trial. This is based in
part on the number of researchers and clinics involved, the size of those
clinics, their catchment areas, the general prevalence of the disease in
question, and the stringency of inclusion/exclusion criteria. In some nutrition
studies, a lone researcher claims to have a trial population far larger than one
could reasonably expect even in a multi-center study, let alone a trial at a
single clinic.
Unusually short recruitment time: Recruiting
patients for legitimate clinical studies is not easy, nor is it swift. It takes
a lot of outreach, effort, and resources. If a study claims to have recruited hundreds
of people with a particular disorder in a 3-month period, and they all met strict
inclusion criteria, you should be suspicious.
Rapid submission & publication: Most studies disclose
the time period for patient recruitment, and the duration of treatment lasted.
From that, you can estimate the earliest possible date of completion. Gaby says
he sometimes sees studies in the nutritional literature that were submitted for
publication very soon after it would be possible to complete the trial, based
on the schedule described in the text.
“In some cases, we’ve seen papers that were submitted before
it was possible to have completed the trial. In many other cases, only a few
weeks to a month after the trial could have been completed. That’s also
implausible, because in a real study, it takes a very long time to analyze
data, to write the paper, and then to submit it.”
An RCT before there is preliminary evidence of
efficacy: Real
clinical trials are costly. Few funding sources are likely to underwrite that
cost without some compelling preliminary evidence from case reports, open-label
uncontrolled trials, or pilot studies showing that the intervention in question
might be beneficial. Yet, in the nutrition and botanical literature, there are
many alleged RCTs done without such preliminary evidence.
Effect sizes larger than one would expect from nutrients: “If you read
a lot of medical literature, you start to get a general idea of how effective
nutrients are. Sometimes it’s dramatic, but most of the time it’s not. Usually,
it’s a combination of nutrients producing a moderate effect,” says Gaby. Yet,
“in many of the studies I’ve looked at, there were much larger effects…effect
sizes you usually only get from drugs. So that raises eyebrows.”
No funding source is listed, or the study is “self-funded”: This is
particularly important when researchers describe their studies as RCTs. Real RCTs
are very expensive. If nobody is funding it, one has to wonder how the study
was possible. And if funding sources are not openly stated, one needs to wonder
why.
The trial design raises ethical issues: If a study involves
patients with serious, advanced disease, and they’re randomized to either a
nutrient or a placebo, there’s likely an ethical problem. That’s because clinical
research is still in the domain of patient care, and doctors have a
responsibility to treat people with the best available therapies. Whether
natural medicine advocates like it or not, the “best available” treatments for
serious diseases are usually prescription drugs. If researchers intentionally
withhold a viable drug option in order to test a nutrient against a placebo,
they’re treading on shaky ethical ground.
Implausible patient characteristics: Pay close
attention to the stated inclusion and exclusion criteria, especially the age
range and baseline characteristics. Dr. Gaby says he sometimes sees papers that
indicate a particular age range for inclusion, but the when he looks at the
mean ages and the standard deviations in the results, it would be
mathematically impossible that all participants actually met the stated age
criteria.
A large study—especially an RCT—authored by a
grad student. Grad
students are the unsung heroes of clinical research. While they certainly
deserve credit for their efforts, the reality of academic hierarchies is that
they are seldom lead investigators, especially on big trials. Yet in the
nutrition literature, one will often see big studies authored by a grad student
or junior researcher, sometimes as the sole investigator. While this is not a
universally damning indicator, it should raise the index of suspicion a bit,
especially if there are other red flags.
Countries
of Origin
Dr.
Gaby says there’s another important indicator of potential scientific fraud:
geography.
“The
most common country of origin, by far, for questionable papers, is Iran. To a
lesser extent, Egypt and China. Then India, Pakistan, Japan, and Italy.”
Though
a German holds first place for total retractions, and other Japanese
researchers aside from Sato and Iwamoto also rank high on Retraction Watch,
Iran is now the world’s leader in terms of the sheer volume of questionable
papers flooding the literature, says Gaby.
“It’s
gotten to the point that if something comes out of Iran, I’m inclined to not
bother even reading it. Which is too bad, because probably some of the studies
are legitimate. But my estimate is that at least three-quarters and probably
more of the studies coming out from Iran these days, and to a lesser extent
from Egypt, Japan, Italy, and others, raise serious concerns about whether the
studies were actually done.”
Iran
has an advanced healthcare
system—a
mix of public, private, and non-governmental non-profit payers. On some public
health metrics, it ranks higher than the US. Roughly 90% of all Iranian citizens
there have some form of healthcare insurance.
Unfortunately,
the country also has a highly competitive market for well-paying, high-prestige
jobs that require advanced degrees and scientific prominence. That, along with
a totally unregulated cottage industry of for-hire study writers, is a major
driver of fraudulent research from Iran.
“The most common country of origin, by far, for questionable papers, is Iran. To a lesser extent, Egypt and China. Then India, Pakistan, Japan, and Italy.”
–Alan Gaby, MD
The
problem is not new. In 2016, Richard Stone the International News Editor for Science
magazine authored an article called, “In Iran, a
Shady Market for Papers Flourishes.” In it, he reveals a lucrative business centered on fabricating
research and getting it placed in the international literature.
For
the equivalent of around $600 (1.8M Iranian Tomans), scientific aspirants can
commission a paper or thesis that ‘doesn’t need lab work.” An additional $400 increases
the odds that the paper will be published “under your own name” in a
“reputable” journal. That means, a journal published by an internationally
recognized publisher like Springer or Elsevier.
“Paper
Mills”
Stone
says there are several thousand of these ‘paper mills’ throughout Iran, mostly
centered around prominent academic institutions. He cites a prominent member of
Iran’s Academy of Sciences who, in 2014, estimated that roughly 10% of all
masters and PhD theses awarded in the country –amounting to about 5,000 theses
per year—are based on research that the candidates never did.
This
is completely legal. There are no laws in Iran—or other countries for that
matter–against fabricating scientific data or publishing bogus research. Stone
notes that in 2016, a group of Iranian scientists concerned about scientific
integrity proposed a law to criminalize—at least partially—the selling of
concocted science. It never saw the light of day.
In
his review in Integrative Medicine, and in his lectures, Dr. Gaby draws
attention to several Iranian researchers who published prolifically on
nutritional topics, and whose work is very likely fraudulent.
Asemi’s
Astonishing Output
Among
them, Zatollah Asemi, a metabolic
disease specialist at the Kashan University, who published more than 191 “RCTs”
over his career, including 148 studies published between Jan 2016 and March
2019.
Zatollah Asemi, MD, an Iranian researcher who has published numerous dietary supplement studies. Many of them do not stand up to close scrutiny. Several have been retracted.
“That’s
almost 50 papers per year,” says Gaby. “Just on face value, that level of
productivity should raise a red flag.”
Further,
Asemi’s output indicates that he was simultaneously running as many as five
RCTs looking at five different treatments, concurrently. “That is unprecented.
In my decades of reviewing scientific papers, I’ve never come across anyone as
remotely prolific as this.”
Asemi’s
numerous citations cover nutrients and herbs including quercetin, ginger,
probiotics, magnesium, zinc, Vitamin D, berberine, and melatonin. He and his
colleagues claim they’ve used these to treat an equally wide range of disorders
including metabolic syndrome, diabetes, depression, leukemia, osteosarcoma, and
polycystic ovary syndrome (PCOS).
Papers
by Asemi and colleagues have found their way not only to obscure open-access
journals, but into some well-reputed high-impact ones like the American
Journal of Clinical Nutrition, the Canadian Journal of Diabetes, and
the British Journal of Nutrition.
Gaby
says the alarm bells about Asemi’s research are loud and numerous.
Beyond
the implausibly prolific output, nearly all of his 191 trials show
unequivocally positive, “statistically significant” outcomes for the
interventions being tested. Often the effect sizes are large—larger than one
usually sees in legit nutrient studies.
Further,
Asemi’s trials often have implausible time lines. “At least 12 of his papers
were submitted to journals before it was possible to have completed the trials.
That’s easy to determine because he says exactly when he started them, and how
long they lasted.”
For
example, a 2018 study of
magnesium and zinc for women with PCOS, published in the journal Biological Trace Elements Research,
states that recruitment was from June to August 2017, and that the treatment
period was 12 weeks. If recruitment ended on August 1 2017, the earliest that a
12-week trial could have been completed would be October 24 2017. Yet the journal
received the paper on Sept 27 2017—weeks before the treatment protocols could
be completed.
“I
looked up some data to see if that was even possible. The region where this
study was conducted (a city called Arak), has a population of about 500,000.
And I looked up the prevalence of gestational diabetes, and the birth rates for
this area. What I calculated was that during any given 3-week period, only
about 36 women in the entire city would have had gestational diabetes between
24 and 28 weeks’ gestation. Yet Asemi claimed to have recruited 60 such women
at just one clinic.”
Reluctance
to Retract
Gaby
shared his concerns about Asemi with the New Zealand team that ultimately took
down Sato and Iwamoto. The group obtained a grant to undertake an exhaustive
review of 172 studies by Asemi and colleagues. The result? A comprehensive
115-page dossier which the Auckland group sent to editors at 65 journals. It
details the myriad inaccuracies, implausibilities, discrepancies, and ethical
breaches spanning Asemi’s career.
Progress
has been slow, but as of now 12 of Asemi’s papers have been retracted, and
editors have issued 85 Expressions of Concern.
Gaby
says there are dozens of other Iranian researchers whose work is just as
questionable. There’s Reza Safarinejad, an internationally known urologist,
whose main interest is male infertility. He’s published numerous studies on the
impact of coenzyme Q10 (ubiquinol) on semen parameters, sperm function, and
pregnancy rates. He’s also published on omega-3s, selenium, and N-acetyl
cysteine for male fertility. According to Gaby, nearly all of Safarinejad’s
studies are problematic.
He points
to one in particular: a 2009 paper in
the Journal of Urology looking at the effect of CoQ10 on sperm parameters and hormone
levels in 212 infertile men.
Safarinejad
is the only author of this paper, and claims to be the sole treating physician.
Gaby holds that 212 is an implausibly large cohort for a stand-alone urology
practice doing its own non-funded research (no funding source is listed). “A
single investigator does not have the time or resources to conduct such a large
trial by himself.”
The protocol
was equally implausible: It claims that all 212 men visited the clinic 12 times
over a period of 13 months, and gave two semen samples at baseline, and two
samples within a 1-2 week period around each visit. Further, the semen was
collected after 3 days of recommended abstinence.
Implausible
Protocols
“That’s
24 semen samples per subject, with a total of at least 72 days of abstinence
over a 13-month period. I don’t know anybody who would do that. If somebody is
infertile and wants to have a pregnancy, he’s going to want to have intercourse
and have a baby. The idea that anyone would sign up for this (protocol) is
crazy,” says Gaby.
There
are also big logistical questions, like the process for collecting the samples.
“While half the 24 semen samples could potentially have been collected during
the 12 clinic visits, the other half (12 samples) would have to be collected
between visits. That is, at home. The subjects would have to deliver the
samples to the clinic within 1 hour of ejaculation, because sperm cells start
to die off after an hour. So, they would have to get to the clinic within one
hour, on 12 different occasions. The paper claims 194 of the 212 men completed
the trial and provided all the required 24 samples. That defies belief.”
Safarinejad
claimed that he and a lab tech did all the semen analyses. Doing the math,
that’s 4,650 sets of lab tests, all of which had to be done within hours of
ejaculation. That’s a heavy workload even for someone not running a busy
clinic.
Further,
the study’s inclusion criteria states that men were eligible to participate
only if they had “normal” fertile female partners “according to investigation.”
That meant the women had undergone a complete medical history, physical exam,
lab testing, and hysterosalpingogram.
“Doing
this on 212 women would be very expensive and time-consuming. It is not
something a urologist would do, so it would be done by a gynecologist. But the
paper does not specify who conducted these fertility evaluations and who paid
for them. And since Safarinejad is the sole author, and there’s no indication
of funding source, it defies the imagination that 212 women would have had salpingograms
just so their husbands could participate in a study.”
Dr.
Gaby sent a letter to the editors of the Journal of Urology detailing
his concerns. “They wrote back by email within 3 hours saying they were going
to investigate this. It took about 6 months, but a couple months ago they
issued an Expression of Concern about all 14 papers that Safarinejad had
published in their journal.” It’s slow progress, but this is several steps in
the right direction.
The
examples cited above are but a few. Gaby says he’s identified many more
problematic studies from Iran and from other countries. And keep in mind that
the US is definitely not immune to bad research.
Corrosion
of Trust
Fraudulent
research corrodes public trust in science; it misleads clinicians; and it skews
metanalyses and systematic reviews. Once marketers and sales people get hold of
it, they easily turn dodgy data into dishonest and misleading product claims.
At minimum, that means ordinary people get ripped off. At the extreme, people
could get hurt.
There’s
no lack of dubious research on pharmaceuticals, but the problem is especially
damaging to the field of natural medicine which is continually fighting for
credibility in the eyes of the broader medical community, the public, and the
regulators. Fraudulent studies like those described in this article bolster the
critics who want to paint the entire supplement industry as dishonest and
maleficent.
As is
easily seen from Dr. Gaby’s experience, and the New Zealand group’s efforts,
medical journals are reluctant to retract studies once they’re published. People
don’t like to admit they’re wrong, and retractions make journals—and their
editors—look bad. Plus, there could be potential accusations of libel, even
lawsuits.
Even
if papers are retracted, their negative impact lingers, especially if they’d
been in the literature for a long time, they appeared in high-impact journals,
and they were included in metanalyses.
Despite
his extensive experience exposing fraudulent research, Dr. Gaby stresses that
most nutrition/supplement researchers are honest, and most studies are clean.
“Most
nutrition research is believable, and the incidents of fraud do not change my
observation that nutritional medicine is highly beneficial for prevention and
treatment of a wide range of health conditions. But this is a stain on
scientific integrity.”
In this webinar, Cory Ambrose, ND, MAT presents the latest research on how to guide your patients through menopause. She discusses the physiological changes that occur during this time, with special attention to the interactions between estrogen and various neurotransmitter systems.
We
will highlight well-researched, novel phytonutrients to help support healthy
hormone and vasomotor balance. These include: spruce lignans, gamma-oryzanol,
taurine, and genistein. We will also explore the importance of nutritional
status, neurotransmitter balance, microbial health, digestion and elimination,
sleep, and stress management during this life stage.
Key
Learning Objectives:
To understand the physiology of menopause from a holistic perspective
Identify micronutrients and botanicals that support the whole body before and during menopause. This includes sleep & stress management, digestion and elimination, nutritional status, and sexual health
Highlight several novel phytonutrients important for healthy hormone balance and vasomotor support (including spruce lignans, gamma oryzanol, genistein)
Understand the role of the vaginal, GI, and oral microbiomes during this life stage
Cory Ambrose, ND, MAT is a Naturopathic Doctor, Educator, and Clinical Science Writer, and is a proud alum of New York University, Bastyr University, and Relay GSE. Dr. Ambrose’s work was shortlisted for the 2021 Digital Education Awards. Dr. Cory is located in Washington state and loves birds, soccer, and reading.
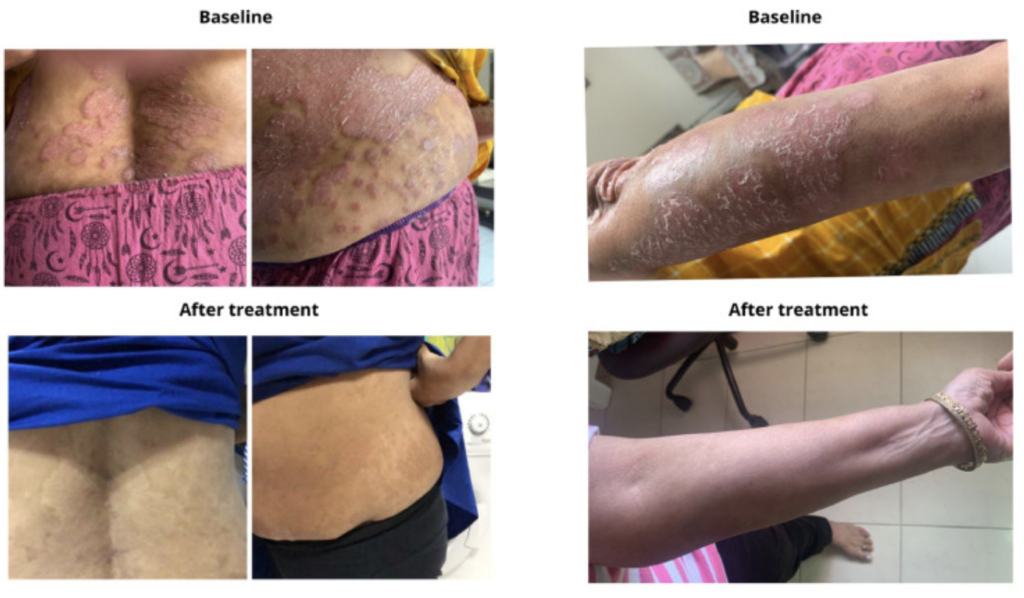
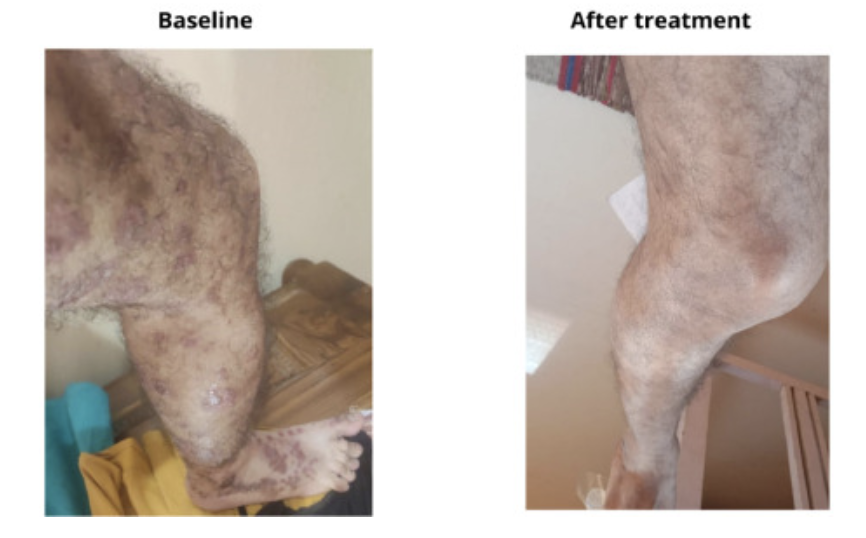
Baseline and post-treatment images of a 58-year-old woman with longstanding psoriasis vulgaris, treated with high-dose vitamin D3 for two months. (Mahtani R, Nair PMK. Clin Immunol Comm. 2023)
A small but
compelling case series published last year suggests that mega-doses of vitamin D can
yield dramatic improvement in the severity of longstanding psoriasis. And by
“mega,” we mean doses as high as 60,000 IU per day.
Renu Mahtani, a physician at the Autoimmunity
Treatment Centre, Pune, India, together with Pradeep M.K. Nair
of the Sant
Hirdaram Medical College of Naturopathy in Bhopal, treated six patients—five
women and one man—with high-dose oral vitamin D (25-hydroxy cholecalciferol)
for periods of 2-6 months, in the absence of other concomitant psoriasis
therapies.
The
patients ranged in age from 48 to 63 years, and all had moderate to severe
psoriasis for between 2-30 years. Three had psoriasis vulgaris, and the others had
the palmoplantar form of the disease.
Prior
to treatment, the physicians measured each patient’s baseline serum vitamin D
levels. Four were within normal range, and they began treatment with 30,000 IU
of oral D3 per day. Two showed severe deficiencies, and began with a one-time
loading dose of 60,000 IU per day, then continued with 30,000 IU per day like
the others.
Every
other month, Drs. Mahtani and Nair measured parathyroid hormone (PTH) levels.
PTH is inversely correlated with serum vitamin D; typically, it is high when
vitamin D is low, and it drops when vitamin D levels rise.
People with psoriasis and other autoimmune disorders sometimes have genetic polymorphisms of the vitamin D receptors which blunt the tissue effects of the vitamin. In other words, they are functionally deficient, though their serum levels of the vitamin may be normal.
They
used PTH changes, along with observations of clinical response, as a guide in
adjusting each patient’s vitamin D dose upward or downward. However, they
cautioned that, “due to the Vitamin D resistance…found in those with autoimmune
disorders, the drop in PTH could be suboptimal, warranting an increase in the
dose of vitamin D to combat this resistance.”
Drs.
Mahtani and Nair also measured ionized calcium levels, as a safeguard against
hypercalcemia which sometimes occurs following prolonged high-dose vitamin D
supplementation.
Obvious
Benefits
The therapeutic
impact of vitamin D was quite impressive, and readily visible even to an
untrained eye.
All six patients showed marked reductions in lesion number, thickness, and severity within 3-6 months of supplementation. The improvements correlated with major reductions in the patients’ PASI (Psoriasis Area and Severity Index) scores.
“Observations
from this case series demonstrate promising and durable control of the signs
and symptoms in psoriasis, with no adverse events or relapse after regular oral
supplementation of Vitamin D3,” wrote Mahtani and Nair (Mahtani R, Nair
PMK. Clin Immunol Comm. 2022).
They
added that adherence to the supplement protocols approached 100%, “as the
patients were motivated by the results.
“Observations from this case series demonstrate promising and durable control of the signs and symptoms in psoriasis, with no adverse events or relapse after regular oral supplementation of Vitamin D3.”
–Renu Mahtani & Pradeep M.K. Nair
A
Key Pathogenic Factor
In
their report, the authors state that many previous researchers have reported
inverse relationships between serum D3 levels and the severity and progression
of psoriasis and other autoimmune disorders.
The
vitamin plays an important role in regulating keratinocytes—the key cells
involved in the pathology of psoriasis. This relationship is also inverse: low
circulating vitamin D levels promote keratinocyte proliferation—the hallmark of
psoriasis—while high blood levels inhibit proliferation (Barrea L, et
al. Rev Endocr Metab Disorders. 2017, Reichrath J. Exper
Dermatol. 2007).
The regulatory
effects of D3 on keratinocytes were initially described by researchers at Osaka University School
of Medicine back in 1990, based on a series of cell culture experiments. Since
then, several human studies have suggested a strong link between vitamin D
deficiency and psoriasis.
In
2012, dermatologist Paolo Gisondi and colleagues at the University of Verona,
Italy, published a year-long, cross-sectional study comparing vitamin D levels
in145 people with chronic plaque psoriasis, 112 with rheumatoid arthritis (RA),
and 141 heathy control subjects.
They
found that the prevalence of deficiency, while high across the board, was
highest among the people with psoriasis—58%, versus 38% among those with RA,
and 30% in the control group. During the winter season, deficiency rates
reached a staggering 81% in the psoriasis group (Gisondi P, et al. Br J
Dermatol. 2012).
Low circulating vitamin D levels promote keratinocyte proliferation—the hallmark of psoriasis—while high blood levels inhibit proliferation.
Dermatologists
at San Cecilio University Hospital, Grenada, Spain, showed that a cohort of 46
people with psoriasis had markedly lower serum 25-OHD levels compared with a
matched cohort of healthy control subjects. The mean values were 30.5 versus 38.3
ng/ml, a statistically significant difference (Orgaz-Molina J, et al. Acta
Derm Venereol. 2014).
Vitamin
D Resistance
But 4
of the 6 patients in the Mahtani-Nair cohort had baseline vitamin D levels
within normal range. This underscores an important point: people with psoriasis
and other autoimmune disorders sometimes have genetic polymorphisms of the
vitamin D receptors which blunt the tissue effects of the vitamin (Zhang F, et al.
Curr Cardiovasc Risk Reports. 2012; Finamor DC, et
al. Dermatoendocrinol. 2013).
In
other words, these people are functionally deficient, though their serum levels
of the vitamin may be normal, and they will likely need markedly higher
supplementation doses to obtain the desired effects.
In
their 2021 review paper, Lemke and colleagues go as far as stating that
genetically-predisposed or acquired vitamin D resistance is a primary
pathologic mechanism for most if not all autoimmune disorders, including
psoriasis (Lemke D, et al.
Front Immunol. 2021).
Topical
calcipotriol and other prescription vitamin D3 analogs have been mainstay
treatments for psoriasis for many years. A 2009 Cochrane Systematic Review of
131 studies concluded that topical D3 analogs are definitely more effective
than placebo ointments, and comparable to the more powerful but side-effect
ridden topical steroids (Mason A, et al. Cochrane Database Syst Rev. 2009).
A
First Line Therapy?
Yet,
despite the apparent connection between systemic vitamin D deficiency and the
etiology of psoriasis, researchers have never seriously explored the
possibility that vitamin D supplementation could be preventive or therapeutic. Mahtani
and Nair contend that theirs is the first case series documenting the safety
and efficacy of high-dose oral supplementation as a treatment for psoriasis.
While
acknowledging that their case series is not a definitive clinical trial, they hold
that it is time for researchers and clinicians alike to take vitamin D
supplementation seriously as a first-line modality for people with psoriasis.
“Optimal
doses of Vitamin D enhances both the natural and adaptive immunity, which makes
this practice effective and worth considering over the present day management
of psoriasis with immunosuppressive drugs,” they write.
Mechanistically,
there’s a strong case to support vitamin D in the management of psoriasis. The
condition is characterized by excessive keratinocyte proliferation
and dysregulated immune activity. Vitamin D appears to modulate both.
Multiple Mechanisms
Deficiency, whether frank or functional, can lead to
unchecked immune activity, contributing to the inflammation and immune
responses typical of psoriasis. The vitamin influences the balance between
regulatory T cells and pro-inflammatory cytokines, which in part determines the
severity of psoriatic lesions.
It is time for researchers and clinicians alike to take vitamin D supplementation seriously as a first-line modality for people with psoriasis.
Mahtani and Nair attribute the dramatic effects they saw,
in part, to the effect of the vitamin on monocytes, macrophages, T cells, and dendritic cells, all of which
play important roles in the etiology of psoriasis.
Vitamin D and
its receptors also influence the integrity of intracellular tight junctions,
which has major implications for barrier function of the skin, and also
potentially, of the gut epithelium.
Visconti and
colleagues at the Sapienza University of Rome showed that the number of vitamin
D receptors was markedly lower in skin tissue samples from 20 people with
psoriasis, compared with samples from normal non-psoriatic individuals. This
correlated with differences in expression of tight junction proteins (Visconti B, et
al. Dermatol & Venereol. 2015).
Safe at High
Levels
In
terms of safety, Mahtani and Nair state that they saw no adverse effects
associated with high-dose oral vitamin D. In 5 of the 6 reported cases, the
patients were able to reduce their daily doses down from 30,000 IU to 20,000 or
even 10,000, after several weeks.
Only
one patient needed a dose increase, from 30,000 IU up to 60,000 for several
months, after which she was able to cut down, in 10,000 IU increments, to a
maintenance dose of 40,000 IU. In this case, the physicians advised the patient
to strictly limit her intake of calcium-rich foods, to avert the possibility of
hypercalcemia.
All
six patients remained recurrence-free, while on maintenance doses of
10,000-40,000 per day. This begs the question of what would happen if they were
to stop their supplementation. It’s an important consideration, and one that
ought to be addressed in future clinical trials looking at the impact of
vitamin D in psoriasis.
The Long Covid nutritional protocol developed by the 10-member practitioner working group under the aegis of OvationLab and ANDHealth, is divided into two parts—Foundational Supplements aimed at improving overall health, and Specialty Supplements focused on the five main drivers of Long Covid: ACE2-mediated tissue damage; viral persistence; chronic inflammation; mitochondrial dysfunction; and microbiome/dysbiosis.
The working group is continually re-evaluating and refining the protocol and dosing schedule.
The
Foundational Supplement protocol includes:
MitoCore (Ortho Molecular Products): a comprehensive multivitamin that also contains N-acetyl cysteine (NAC), Glucoraphanin, Alpha lipoic acid (ALA), Resveratrol, Epigallocatechin gallate (EGCG), Acetyl L-carnitine, Manganese, and Zinc. The working group recommends 2 caps, twice daily for 90 days.
OmegaGenics (Metagenics), a concentrated Omega-3 product containing 710 mg EPA and 290 mg DHA; 1,000 mg twice daily for 90 days.
Magnesium Glycinate, 200 mg twice daily for 90 days
Co-Enzyme Q10, 200 mg per day, for 90 days
Quercetin, 500 mg, twice daily for 90 days
Vitamin K2 with D3: Up to 10,000 IU daily, with specific dosing based on each patient’s serum levels. If the serum level is below 40 ng/ml, use 10,000 IU. If it’s within 40-60 ng/ml, use 5,000IU. If above 60 ng/ml, the patient does not need supplementation.
The
Specialty Supplement protocol consists of:
Arterosil (Calroy Health Sciences): The main
constituent in Arterosil is Rhamnan sulfate,
a
sulfated polysaccharide from two types of marine algae (Monostroma
Latissium and Monostroma Nitidum). Rhamnan sulfate has a similar
structure to glycosaminoglycans found in the human endothelial glycocalyx—the thin
gel-like layer that coats the luminal surfaces of healthy blood vessels. Glycocalyx
damage is
one of the earliest steps in the pathogenesis of cardiovascular disease, and it
is a
common consequence of Covid.
“In
order to have any hope of repairing tissue damage, we need optimized blood flow
and optimized vessel health. Arterosil targets the regeneration and repair of
the endothelial glycocalyx,” said Kristine Burke, MD, a co-chair of the PVRP
Working Group, during a
webinar outlining the protocols.
ITIS (Return
Healthy): This product is a
complex of anti-inflammatory herbs, including Skullcap (Scutellaria
baicalensis), Curcumin (Curcuma longa), Frankincense (Boswellia
serrata) and others. Dr. Burke noted that Scutellaria produces a compound
called Baikalin that is able to cross the blood-brain barrier, making the
product useful for mitigating the cognitive impairment, mood disturbances, and
“brain fog” that many Long Covid patients experience. That’s in addition to the
product’s capacity to reduce systemic inflammation, one of the main drivers of
the post-viral syndrome.
Tollovid (Todos Medical): This unique substance is derived from an herb
called Lithospermum erthythrorhizon, known colloquially in English as
Gromwell root, or Zicao in Traditional Chinese Medicine.
“Tollovid
addresses persistent viral infections by blocking viral replication capacity,”
explained Dr. Burke.
It does this by binding tightly to the 3CL protease, an enzyme that coronaviruses use to cleave the long polypeptide chains produced from their mRNA during the replication process. Tollovid is among a number of 3CL inhibitors being explored in the Covid context. Essentially, it shuts down the replication process.
MegaSporeBiotic (Microbiome Labs): This probiotic
product delivers spores from five strains of Bacillus subtilis. PVRP
Working Group members believe it is ideally suited to address the marked
microbiome alterations associated with Covid and sometimes, Covid vaccination.
“We want to recondition the gut and bring back a healthier microbiome,
especially facilitating the resurgence of those species that are important in
immune regulation,” Burke said.
Rather than “seeding” the gut with exogenous probiotic organisms, the goal of treatment with a spore-based product like this is to shift the microbial ecology so that it favors growth and flourishing of a patient’s own endogenous bacterial species.
MegaPre (Microbiome Labs): A prebiotic product containing three different types of non-digestible oligosaccharides derived from kiwi fruit, nonGMO corn cobs, and rBST-free cow’s milk. Supplementation with this combination increases GI microbial diversity and selectively feeds beneficial organisms like Akkermansia muciniphilia, Faecalibacterium prauznitzii, and various species of Bifidbacteria which, Dr. Burke noted, are often decimated by SARS-CoV-2 infection.
“We found ourselves needing a curated suite of nutritional product solutions that were targeted at the five main drivers of Long Covid: ACE2 mediated damage/tissue damage; viral persistence; chronic inflammation; mitochondrial dysfunction; and microbiome/dysbiosis.”
–Kristine Burke, MD
For
the first 30 days, in addition to the full array of Foundational supplements,
patients should take: Arterosil, 2 caps twice daily; ITIS, 2 caps thrice daily;
Tollovid 3 caps 4 times per day; and MegaSpore alone (the prebiotic is added
later), 1 cap daily for the first 7 days, and then 2 caps daily until the
bottle is finished.
From Day 30 to Day 90, patients can cut the doses to: Arterosil 1 cap twice daily; and Tollovid 1 cap twice daily for 30 days. They should eliminate the MegaSpore probiotic, replacing it with the MegaPre oligosaccharide formula, 3 caps per day.
All products in the protocols are available as a bundle from Fullscript. Practitioners with Fullscript accounts can prescribe the complete protocols for patients, and Fullscript will deliver the full product suite to their homes, along with detailed implementation instructions.
Dr.
Burke and members of the Working Group stress that the current protocols,
though based on a scientific review of hundreds of potential candidate products,
are still a work in progress. The team has established a standardized registry
to track outcomes in hundreds of patients now on the protocols, and they will
use the data to revise the protocols if necessary.
She
added that these regimens are flexible. “There may be some patients for whom we
want to add some other tools not on the protocol list. You may choose to add or
subtract products. But this is the broadest and simplest set of products and
processes that we could develop. We’re not promoting specific brands
necessarily. But the ones on the list, we found data to support the use of each
of them to target one or more of the five key drivers of long Covid.”
Disclosure: ANDHealth and Calroy Health Sciences are clients of OvationLab.
Autoimmunity and gastrointestinal disorders are inter-related
and increasingly common problems. Because the different autoimmune diseases affect
specific organ systems, patients are often shunted to specialists who approach
these conditions through their relatively narrow specialty lenses.
Though they may manifest differently, most autoimmune diseases
have the same common triggers. If we know what causes the immune system to
attack itself and we can identify some of the triggers causing a malfunction in
the immune system, we can successfully treat many seemingly different disorders
using a similar approach.
In this free webinar, Michael Jurgelewicz, DC, CNS, will discuss
an integrated treatment approach for autoimmune and gastrointestinal disorders,
using case studies from his own clinical practice to illustrate the key points.
You’ll learn about:
How to identify environmental triggers that contribute to autoimmunity
The role of clinical laboratory testing to assess autoimmune dysfunction
Comprehensive molecular evaluation of the gut microbiome, gut inflammation, mucosal immunity, and digestive function.
Assessment of opportunistic bacterial, protozoal, and viral pathogens, as well beneficial microorganisms organisms
Dietary interventions and nutritional therapies for patients presenting with autoimmune disorders
Michael Jurgelewicz, DC, DACBN, DCBCN, CNS is the founder and director of Bucks County Center for Functional Medicine in Yardley, PA. He specializes in functional medicine in the management of a variety of chronic health conditions. In addition to his chiropractic degree, he is a Certified Nutrition Specialist, board-certified in nutrition by the American Clinical Board of Nutrition, and a Diplomate of the Chiropractic Board of Clinical Nutrition. He is also a member of the American Clinical Board of Nutrition’s Item Writer’s Committee and is the author and contributor to several professional publications. Dr. Jurgelewicz is the Director of Product Development, Research, and Clinical Support for Designs for Health, Inc.
Should people
with Health Savings Accounts (HSAs) be permitted to use their tax-deferred
dollars to buy dietary supplements and herbal medicines?
It’s a question
that will once again confront members of Congress in the months to come.
Under current
federal tax rules, supplements are excluded from HSAs and also from Flexible
Spending Accounts (FSAs), unless they are explicitly prescribed by physicians. Over
the years, self-care advocates and supplement industry trade groups have
challenged that policy, to no avail.
Now, it appears the idea has found some new congressional allies.
On July 20, Rep. Darin LaHood (R-IL), son of longtime conservative stalwart Ray LaHood, introduced a new bill titled the Dietary Supplements Access Act, calling for amendments of the federal tax code that would include all types of supplements in HSAs and FSAs. LaHood has a senior position on the influential House Ways and Means Committee, which will likely have influence on the future of the bill.
LaHood’s co-sponsors are Reps. Brendan Boyle (D-PA) and John Curtis
(R-UT), and John Gottheimer (D-NJ), a coalition that suggests the proposition
has a fair degree of bipartisan support.
Rep. Darin LaHood (R-IL) introduced a new bill to include supplements in HSAs & FSAs.
According to
Patricia Knight and Peter Reinecke, political advisors to the UNPA, more than
35 million Americans have tax-preferred HSAs, representing over $100 billion. An additional 21 million people have FSAs through
their employers.
UNPA and the other industry organizations contend that the longstanding exclusion of supplements as an eligible expenditure denies HSA and FSA-holders full freedom of choice, and reflects a nonsensical bias against one of the cornerstones of a healthy lifestyle.
A Strong Case
On June 21, Steve
Mister, CEO of the Council for Responsible Nutrition, along with executives
from several member companies, met with representatives on both sides of the
political divide to advocate for the new bill which, if made law, would
include, “everything that has a ‘Supplement Facts’ box on the label” as an
eligible FSA/HSA expense.
In an interview
with Nutraingredients
USA,
Mister said he was optimistic about the future of the proposal.
The new bill is
essentially the same as the Dietary
Supplements Access Act
(HR 5214), introduced in
2021 by Rep. Curtis. It declares all vitamin, mineral, amino acid, and
botanical supplements to be eligible expenses.
HR 5214 failed
to make it past the House Ways and Means committee in 2021.
Mister says CRN
and other industry groups have done a lot of homework since then, and he feels
they are now much more able to make a strong case.
Broad adoption of evidence-based supplementation strategies for six conditions—coronary artery disease, osteoporotic fractures, age-related macular degeneration, irritable bowel syndrome, and childhood cognitive disorders—could potentially cut over $400 billion from the nation’s medical bill by 2030.
Addressing Objections
Congressional objections to the proposal tend to fall into two general categories.
Steve Mister, CEO, Council for Responsible Nutrition
Some lawmakers view HSAs and FSAs as “tools for rich people as tax dodges,” he explained. They tend to view any expansion of HSA/FSA benefits as further opportunity for wealthy people to avoid paying their fair share.
To
redress this perception, he points to a survey of HSA/FSA holders showing that,
“the vast majority of people using these accounts are not wealthy
“one-percenters,” but rather, ordinary middle-class working Americans.
Further,
the survey showed that
78% of the 1,100-plus account holders want to be able to use their tax-exempt
healthcare savings to purchase supplements.
“They
want that flexibility. They want to be to do things that are more proactive on
healthcare, and not just use their HSA reimbursements for co-pays on doctor
bills and prescriptions when they’re sick,” Mister told NutraIngredients.
78% of the 1,100-plus account holders surveyed want to be able to use their tax-exempt healthcare savings to purchase supplements.
The
other major congressional objection is the belief that expanding HSA/FSA
benefits would encourage diversion of more money away from taxable income
streams, which would negatively impact the national treasury.
To
this, Mister cites data showing that in reality, peoples’ decisions about
FSA/HSA allocations come down to how much they believe can afford to take out
of their paychecks, which is typically not that much. Tax avoidance is rarely a
driving factor.
Potential Cost Savings
He
contends that measures to encourage wider use of supplements would lead to
long-term, system-wide cost savings.
A
2022 study called Supplements to
Savings
indicates that broad adoption of evidence-based supplementation strategies for
six conditions—coronary artery disease, osteoporotic fractures, age-related
macular degeneration, irritable bowel syndrome, and childhood cognitive
disorders—could potentially cut over $400 billion from the nation’s medical
bill by 2030.
Data like that, Mister says, should be able to win over the nation’s elected officials. “In so many places, government is paying for healthcare—whether it’s VA benefits, or Medicare, or Medicaid. They’ve got a real interest in lowering healthcare costs. So, with all of that together, we had a pretty compelling argument.”
It remains to be seen whether the cost-savings argument will
prevail in a gridlocked, highly partisan congress bent on “fiscal restraint,”
as UNPA’s political advisors have termed it. Knight and Reinecke note that the
influential Joint Committee on Taxation (JCT), which rates the budgetary impact
of all tax-related legislation, has in the past scored proposals for supplements
in HSAs as a net cost, not a savings, for the government.
Advocates for the revision are urging practitioners, patients, and
any other interested parties to call or write to their congressional
representatives and urge them to support and co-sponsor the bipartisan Dietary
Supplements Access Act.
A Push for Vitamin D
The HSA/FSA campaign is not the only current attempt to crack the
federal government’s intransigent attitude toward supplements.
Earlier this year, a coalition of nutrition advocacy groups led by the Organic & Natural Health Association (ONHA) is urging Congress to include vitamin D as an eligible expense under the federal Supplemental Nutrition Assistance Program (SNAP).
Crystallograph of Vitamin D3 (cholecalciferol). Image by Michael Davidson, Optical Microscopy Division, Florida State University
Dietary supplements,
including vitamin D, are excluded from SNAP, aka “Food Stamps,” and from other
federal healthcare programs.
“Permitting more low-income citizens to buy vitamin D with SNAP will ultimately reduce the burden of chronic disease, cut healthcare expenditures, and save taxpayer dollars.”
–Karen Howard, Executive Director, Organic & Natural Health Association
ONHA and its allies
are working to
change that by rallying health-conscious citizens, nutrition industry
representatives, and medical professionals, to urge their elected officials to
amend the Farm Bill which governs SNAP, to allow recipients to purchase vitamin
D using their SNAP dollars.
An Affordable
Solution
“Vitamin D3
supplements offer an affordable solution to address a range of health
challenges faced by families, including preterm births, depression, respiratory
infections, asthma, cancer, and chronic diseases like cardiovascular issues,
high blood pressure, and Type 2 diabetes,” says Karen Howard, ONHA’s CEO, in a statement announcing the advocacy campaign.
Karen Howard, Executive Director, Organic & Natural Health Association
Permitting more low-income citizens to buy vitamin D with SNAP will ultimately reduce the burden of chronic disease, cut healthcare expenditures, and save taxpayer dollars, says Howard.
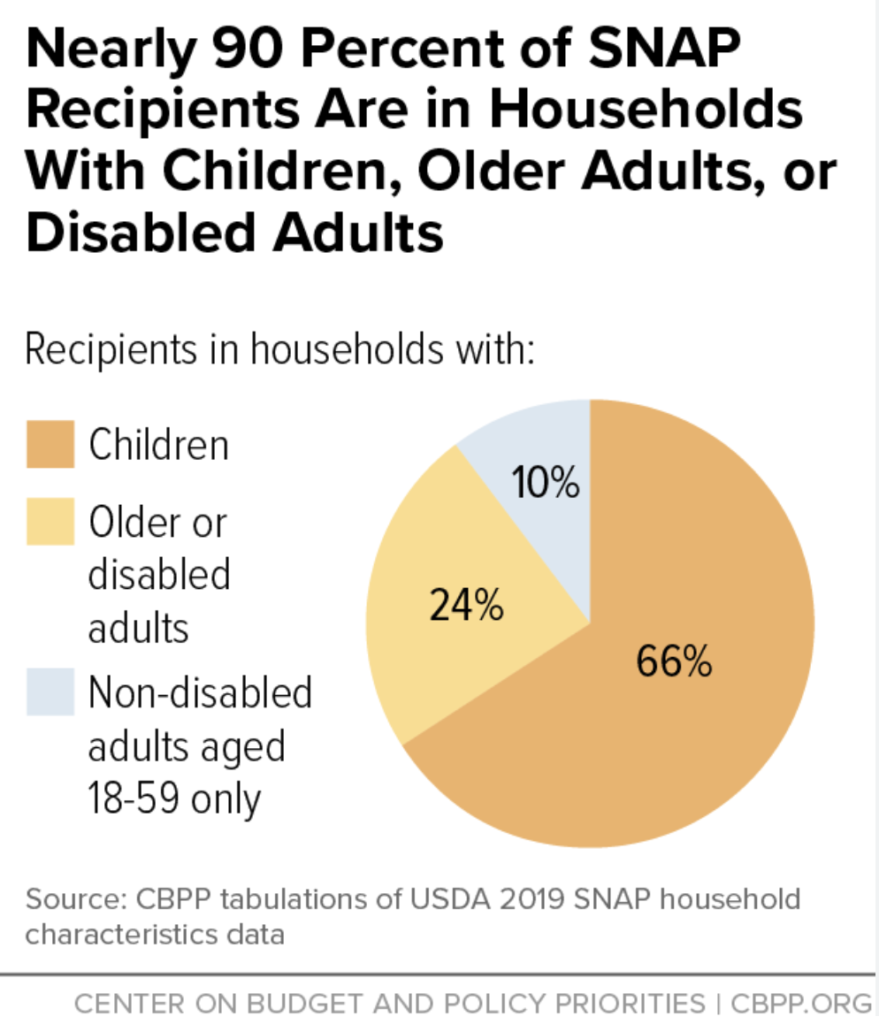
Over 41.2 million Americans—roughly 12% of the US
population—are now enrolled in SNAP, which was born out of federal food
assistance programs created during the Great Depression in the 1930s. The
modern SNAP program’s stated intention is to provide “food benefits
to low-income families to supplement their grocery budget so they can afford
the nutritious food essential to health and well-being.”
Cruel Irony
In
practice, a lot of products that people can buy using SNAP are very far from
“nutritious” or “essential to health.”
Soft drinks,
cookies, cakes, and a wide variety of nutritionally-void junk foods are
considered “eligible” under existing SNAP rules. According to a 2016 report by
the US Department of Agriculture, sodas are the top most-purchased commodity by SNAP beneficiaries.
All for Vitamin
D’s leaders
point out that, “While
SNAP permits the purchase of a diverse range of foods, encompassing fruits,
vegetables, grains, dairy, and proteins, it lacks explicit guidelines
concerning the quality and nutritional value of these items.
When it comes
to meeting therapeutic vitamin D levels (40-60 ng/ml), SNAP falls short,
especially since it is very difficult to obtain these levels solely via food or
sunlight exposure. This is doubly true for dark-skinned people, who represent a
disproportionate number of SNAP recipients.
In practice, a lot of products that people can buy using SNAP are very far from nutritious. Soft drinks, cookies, cakes, and a wide variety of nutritionally-void junk foods are considered eligible under existing SNAP rules. Supplements are excluded as “non-foods.”
An Ongoing
Effort
The All for
Vitamin D campaign is the latest step in a long, arduous
effort to
convince lawmakers to expand SNAP’s definition of “food.”
In 2017, Rep. Mike Rogers, an Alabama Republican, introduced the SNAP Vitamin and Mineral Improvement Act which would have modified the program to include a broad range of vitamins, minerals, and other supplements as an eligible expense.
Rogers’ bill
had strong support from nutrition industry trade groups, as well as some
high-profile policymakers, and was included in the House version of the 2018
Farm Bill. But was killed in the Senate, despite strong advocacy from longtime
supplement advocate, Sen. Orrin Hatch.
At the time Senate
agriculture committee chairman Pat Roberts (R-KS) and ranking Democrat Debbie
Stabenow (D-MI) opted to cut all Farm Bill amendments that might be perceived
as partisan obstacles to smooth passage. The committee deemed Rep. Rogers’ proposal
as one of those obstacles, and nixed it from
the final 2018 version.
Under SNAP’s
current rules, vitamins and supplements are considered “non-food” and therefore
ineligible for purchase with SNAP dollars. Policymakers justify the exclusion, arguing
that if beneficiaries can use SNAP coupons for supplements, they will divert
their limited funds away from “real” food. That’s ironic given the myriad junk
foods and beverages now covered by the program.
Further, the
notion that everyone can derive all important nutrients directly from food, and
that supplements encourage people to skip “real” meals, ignores the fact that many
people relying on SNAP and other forms of food assistance already miss meals simply
because they don’t have enough to eat.
The average SNAP benefit equals around $4 per person per day, or approximately $1.40 per meal. That doesn’t go very far given today’s food prices.
By playing to the strong science on vitamin D, the widespread prevalence of deficiency, and the staggering scope of food insecurity, ONHA and its allies have a fighting chance to win the minds and hearts of some lawmakers.
Missed
Opportunities
Outside of SNAP, many other food assistance programs such as local food banks and food pantries also exclude supplements.
The number of people visiting food banks, already high before Covid, has soared since the pandemic. Three years on, 80% of food banks still report either an increase in or a steady demand for emergency food relief month-to-month, according to Feeding America. Nationwide, food banks and related programs are serving 55% more people than before Covid. According to the organization, Feeding America, at least 60 million Americans visited food banks last year.
The average SNAP benefit equals around $4 per person per day, or approximately $1.40 per meal. That doesn’t go very far given today’s food prices.
As is the case
with SNAP, many people who rely on community pantries are unlikely to get all
the nutrients they need through diet alone. Yet these programs do not provide
dietary supplements.
Administrators
at food banks say they often receive donations of supplements from retailers,
distributors, food drive collections, and manufacturers. But these products
create a real conundrum. On one hand administrators recognize their potential
for improving nutritional status, but on the other they are aware of issues like
purposeful or
accidental adulterations and exaggerated product claims.
There are no
established standards for evaluating the safety and potential benefits of
supplements, so food bank staffers—who are typically overwhelmed by the sheer
number of people they must serve–are left to their own judgment in deciding
whether or not to distribute supplements.
Supplements are not the ultimate answer to poor nutrition among the nation’s poorest citizens. But they could be important tools in helping people move toward better overall health.
In 2019, a
national program called Healthy Eating
Research
(HER) convened an expert panel “to improve the quality of foods in food banks
and pantries in order to increase access to and promote healthier food
choices.”
The group
issued a final report in March 2020
entitled, Healthy
Eating Research Nutrition Guidelines for the Charitable Food System.
The guidelines acknowledge the existence of dietary supplements, grouping them
among protein powders, baby food, and other “miscellaneous items” that are “considered
necessary only for specific populations or when treating specific disease
states.”
Though HER does
not categorically dismiss supplements, it definitely counsels against wide use,
and does not provide practical guidelines for food pantry administrators.
The reality is,
supplement products rarely make it to the pantry shelves.
Vitamins, minerals, and other supplements are not the ultimate answer to poor nutrition among the nation’s poorest citizens. But they could be important tools in helping people move toward better overall health.
A recent study of data from more than 19,000 people showed that those who experience multiple sites of chronic pain are more likely to show hippocampal atrophy than those who are pain-free. The brain changes correlated with cognitive decline. (Image: Master1305/Shutterstock)
A massive new study of data from over 19,000 individuals shows
that chronic pain is associated with loss of hippocampal volume and increased
risk of dementia.
Compared with pain-free control subjects, those who had five
or more areas of chronic pain showed neurological changes equivalent to eight
years of excess brain aging (Zhao
W, et al. PNAS. 2023). Simply put, the more regions of chronic
pain people experience, the greater their risk of neurocognitive abnormalities.
“Our results suggested that cognitive decline and
hippocampal atrophy interact biologically and may underlie the increased risk
of dementia associated with multi-site chronic pain (MCP),” write Zhao and
colleagues, based at the CAS Key Laboratory of Mental Health, Chinese Academy
of Sciences, Beijing.
Zhao’s team used data from the UK Biobank,
concentrating specifically on files from more than 19,000 individuals who’d
undergone brain scans. The chronic pain problems in this large cohort were the
result of a wide variety of causes, including arthritis, cancer, and low back
pain.
Regardless of the specific causes, the brain impact of
chronic pain was consistent.
“We found that individuals with MCP were associated with
significantly higher dementia risk, broader and faster cognitive impairment,
and greater hippocampal atrophy than both pain-free (PF) individuals and those
with single-site chronic pain (SCP),” the authors note.
The impact of chronic pain on hippocampal volume and
dementia risk correlated strongly with number of coexistent chronic pain sites,
and the observed hippocampal atrophy was associated with measurable declines in
fluid intelligence.
“Our results suggested that cognitive decline and hippocampal atrophy interact biologically and may underlie the increased risk of dementia associated with multi-site chronic pain (MCP)”
—Wenhui Zhao, Institute of Psychology, Chinese Academy of Sciences, Beijing
In other words, constant pain in multiple anatomical sites leads
to detrimental brain changes and impairs cognitive function.
One in Five
These findings should prompt physicians in this country to sit
up and pay attention.
In its April 14, 2023 edition of Mortality and Morbidity Weekly
Report, the CDC estimated that fully one
in five adults– approximately 20.9%, or 51.6 million people—experienced chronic
pain in 2021, with 6.9% experiencing intense pain that limited daily
activities.
Those numbers are telling us something: conventional
medicine, with its limited tool kit for managing pain, is not doing a very good
job.
Most physicians rely on NSAIDs, acetaminophen,
antiepileptic drugs, and serotonin/dopamine agents when treating people who
live with chronic pain. Or they refer these patients out for surgery. The stats
from the CDC and other sources show us clearly that this isn’t working. And in light of the Zhao study, our system’s
failure to properly address chronic pain has long term negative implications
for cognitive health.
This article will review three key areas:
A
quick overview on how we can do better in eliminating pain
Key
tools for preventing dementia in general
Use
of low-dose naltrexone (LDN) to prevent pain-induced dementia
Secrets to Pain Relief
People do best with a comprehensive approach to pain
management. This means addressing:
The biochemistry of pain, via diet and nutrient
interventions, herbs, and in some cases, prescription medications
The structural components of pain, via osteopathy,
myofascial release, and chiropractic
Mind/body/spirit aspects of pain, via
techniques to release old emotions stored in muscles and the brain, and by eliminating
things that are a “pain in the back” (or even lower!)
We will focus here on the biochemistry of pain relief, and
dementia prevention.
Why Do We Have Pain?
The first step in eliminating pain is to realize that pain
is not meant to be an enemy. Rather, it is like the warning light on a car’s
dashboard telling us that something needs attention.
(Image: Passakorn vejchayachai/ Shutterstock)
When someone’s “oil light” goes on, in the form of a
chronic pain, the standard medical response is to prescribe a drug or undertake
a surgical procedure to make the warning signal disappear. And then, when the patient’s
“motor” burns out, they think it was just coincidence.
But what if, instead, we treated the flashing oil light by actually
adding oil? This works wonderfully!
What is Pain Asking For?
There are several pain-associated biochemical warning
lights that are asking for different things. The most common ones are:
Low tissue energy: When muscles don’t have
enough energy, they get locked into shortened positions, causing pain. It takes
more energy for a muscle to relax, than to contract. This may seem
counterintuitive, but consider how your muscles feel after a heavy workout. They
don’t go loose and limp, rather they become tight. Chronic low tissue energy
causes myofascial pain, and this is present in most cases of chronic pain, even
if it is not the original cause of the pain.
Inflammation or immune imbalance: This
is generally present in all conditions that end in “-itis,” such as arthritis.
It is also present in many autoimmune illnesses. For arthritis, the herbal mixture
Curaphen was as effective as Celexicob in head-on studies. Glucosamine and
chondroitin was also highly effective, likely by feeding the joints the
substrates they need to build and maintain cartilage.
Nerve pain: Interestingly, this is
associated with uncontrolled firing of pacemaker-like cells, which then also
deplete energy. Common triggers include nutritional deficiencies, low cellular
energy from diabetes, fibromyalgia or hypothyroidism, and infections. Lipoic
acid, 300 mg, twice daily and Acetyl-L-carnitine, 1000 mg, can be helpful in
mitigating nerve pain, though it usually takes at least three months of regular
use.
Central or brain pain: This is triggered by
most other types of chronic pain, and it is associated with microglial
activation (discussed below). Shutting down the microglial activation with
low-dose naltrexone or other treatments can be very beneficial.
Sympathetically Maintained Pain/Complex Regional Pain
Syndrome (CRPS): According to the International Association for
the Study of Pain, sympathetically maintained pain is, “a type of pain that is
maintained by sympathetic efferent innervation or by circulating catecholamines.”
It can occur by itself or in conjunction with other types of pain. CRPS,
formerly called “Reflex Sympathetic Dystrophy” is one form of it. This can be
extremely debilitating. Management of CRPS is beyond the scope of this article
but suffice to say the condition is now treatable. Feel free to email me at fatiguedoc@gmail.com
for a CRPS information sheet outlining my approach.
The CDC estimated that fully one in five adults experienced chronic pain in 2021. The numbers are telling us something: conventional medicine, with its limited tool kit for managing pain, is not doing a very good job.
Basics for Pain Relief
In general, when treating chronic pain, I start with general
nutritional and herbal support.
Especially important is to ensure that the patient is
getting high levels of B vitamins and magnesium to restore tissue energy. Then,
omega-3s and herbs to balance inflammation. For the omega 3 support I use
EurOmega 3, as one pill replaces seven large fish oil pills or capsules. I also
then add Curaphen1-2 caps 3 x day. This pain relief formula contains a unique
highly absorbable form of curcumin to balance cyclooxygenase (COX), boswellia
to balance lipoxygenase (LOX), DL phenylalanine (DLPA) to increase endorphins,
and nattokinase to mitigate inflammation and oxidative stress.
For arthritis or traumatic pain, I add a topical Comfrey (Symphytum)
cream three times a day. Give this and the Curaphen for six weeks to see the
full effect. These products can be combined, and also taken with other pain medications.
It is remarkable how much research shows that the
risk of dementia can be dramatically decreased via
nutritional, botanical, and lifestyle interventions. And conventional medicine largely
ignores all of this because the treatments are not expensive pharmaceuticals.
There are many things that can help. Here are some basics,
organized around the mnemonic “MIND”:
METABOLIC- The
key here is to optimize hormone levels with bioidentical hormone therapies. For
example, thyroid
hormone levels are strongly associated with risk of
dementia. But there are gender differences in how this relationship plays out.
In women, low-normal thyroid levels are associated with a 240% higher risk of
dementia. In men, borderline elevated thyroid levels raise dementia risk by
800%!
Testosterone
levels also influence risk of dementia, with low testosterone
increasing it while higher levels seem to be protective. A 50% increase in free
testosterone in the bloodstream was associated with a 26% decrease in the risk
of Alzheimer’s. Men who develop Alzheimer’s disease have about half the free
testosterone in their bloodstreams as men who do not.
INFECTIONS- Always
check for silent bladder infections. Also consider candida, if a patient is
experiencing a lot of postnasal drip, throat clearing, or flatulence. Chronic
infections are associated with increased risk of dementia.
NUTRITIONAL Support- Beyond
the basics of a healthy plant-rich diet, and the support of a good multivitamin,
it is important to optimize folate, B12, other B vitamins, and Vitamin D.
When working with chronic
pain patients, always check the B12 level. You want to keep that over 540 ng/L.
Also look at the homocysteine level. Ideally, that should be under 9 µmol/L. The value of B vitamins in preventing
dementia have been shown in a number of studies. For example, in the 2012 VITACOG study, people with mild cognitive impairment who
took a daily
combination of 0.8 mg folic acid, 0.5 mg vitamin B12, and 20 mg vitamin B6
showed markedly slower rates of cognitive decline and less brain atrophy than
those assigned to the placebo group.
VITAMIN D is also very important, as was shown in a prospective study of over 12,000 individuals published earlier this year. Researchers at the University of Calgary found that, “Across all formulations, vitamin D exposure was associated with significantly longer dementia-free survival and lower dementia incidence rate than no exposure.”
In the population as a whole, taking vitamin D was
associated with a 40% lower incidence of dementia. The effect was significantly
stronger in females versus males. It was also greater in those who had normal
cognition at baseline compared with those who already had some degree of
cognitive impairment.
Likewise, the protective effect seemed stronger in
non-carriers of the apolipoprotein E ε4
allele versus carriers of this risk factor.
Be careful with iron,
especially in carriers of the apolipoprotein E ε4 allele. According to researchers at the
University of Melbourne,
the presence of this gene tends to elevate ferritin levels in cerebrospinal
fluid, and this is associated with declines in cognitive performance and
increased risk of developing Alzheimer’s disease.
Do not supplement with iron
if someone’s ferritin level is over 60 µg/L.
Curcumin
(turmeric), a culinary favorite, appears to be neuroprotective. It is notable
that the prevalence of
Alzheimer’s in India—where curcumin is a dietary mainstay– is 70% lower than
in the US. Curcumin also shows promise in many neurodegenerative conditions,
including Parkinson’s.
Supplementation with
curcumin makes sense for people at increased risk of cognitive decline. But
this is one herb for which the form and brand really matter. I recommend a highly
absorbable form of Curcumin called CuraPro, 750 mg, twice daily.
Be Cautious with Meds
Yes, pharmaceuticals are sometimes necessary for prevention or treatment of serious illnesses. There’s no question that drugs to control blood pressure, especially beta blockers and ACE inhibitors, can be protective for the brain in patients who have hypertension.
But it is equally important
that we get our patients off unneeded or harmful drugs as often as we can.
Avoid Proton
Pump Inhibitors: In a 2016 study of over 73,000 elderly
individuals, taking a PPI such
as
omeprazole and pantoprazole was associated
with a 44% increase in dementia risk. Famotidine, an H2
receptor antagonist, does not seem to carry a similar risk.
Avoid Anticholinergic Drugs: Diphenhydramine, tricyclic antidepressants, and
incontinence drugs like oxybutynin and tolterodine are especially problematic. In
a study of 451 older individuals, cognitively normal at baseline, the use of
anticholinergic drugs markedly increased risk of brain atrophy and cognitive
impairment. The risk increase begins with as little as 60 days’ exposure.
Low-Dose Naltrexone
As noted at the beginning of this article, chronic
pain is associated with decreased brain volume and increased dementia risk.
I believe low-dose naltrexone (LDN)—an old and
inexpensive therapy–could potentially prevent millions of cases of dementia by
alleviating chronic pain. Why? Because LDN addresses one of the main drivers of
both chronic pain and brain atrophy.
Numerous studies show that microglial activation is a common denominator between chronic
pain, fibromyalgia, and shrinking brain size. Researchers now recognize that
microglial activation could be a potential target for pain management.
Microglial cells can be viewed as the brains
“gardeners.” Normally they are mild-mannered, and simply tend to the needs of
brain cells. They provide a first line of immune defense, and they are
constantly “weeding” the brain of damaged neurons or potentially problematic
amyloid buildup.
But when something goes amiss in the brain, such
as a viral infection or a chronic pain problem, these mild-mannered gardeners can
become overactive and they start damaging healthy brain tissue. This microglial
activation contributes to brain shrinkage and decreased volume.
The remedy? LDN!
At doses of 3-5 mg per night, LDN turns off
microglial activation. This approach was outlined in a
2019 paper by Diana Trofimovitch and Steven Baumrucker, who propose the off-label use of LDN to
manage non-malignant pain. “When used in doses of 1 to 5 mg, it acts as
a glial modulator with a neuroprotective effect via inhibition of microglial
activation.”
LDN has been shown in numerous studies, and borne out by wide clinical experience, to help eliminate pain and other debilitating symptoms of chronic pain conditions. There is a high probability that by shutting down the microglial activation, it can also prevent the increased dementia risk associated with chronic pain (See Low-Dose NTX to Quell Chronic Pain & Lower Risk of Dementia)
For information on how to treat fibromyalgia, long Covid
symptoms, and other chronic pain syndromes, feel free to email me at FatigueDoc@gmail.com and
ask for my free information sheets. Please let me know that you are a
practitioner, so I can include the free treatment questionnaires and
checklists.
For guidance on how to address each type of pain (e.g.,
arthritis, migraines, etc.) simply download the Cures A-Z smartphone app. This
tool quickly reviews each of the most common health conditions and suggests the
best natural and prescription therapies for them. It’s kind of like having my
brain in your pocket – but less messy!
END
Jacob Teitelbaum, MD, is one of the most frequently quoted
integrative medical authorities in the world. He is the author of several
best-sellers, including From Fatigued to Fantastic!, the Beat Sugar Addiction
Now! series, The Fatigue and Fibromyalgia Solution, and the popular free
smartphone app Cures A-Z. He is the lead author of 4 studies on effective
treatment for fibromyalgia and chronic fatigue syndrome. He earned his MD
degree from Ohio State University, and recently celebrated his 50th
year as a physician. Learn more at Vitality101.com.
Intermittent fasting—a meal schedule that alternates between normal eating patterns and brief but frequent full fasts (or restricted caloric intake)—is an effective method for stimulating autophagy and improving immune system resilience (image: Sendo Serra/ Shutterstock).
The following article is excerpted and adapted
from the new book, Immune Reboot: Your Guide to Maximizing Immunity, Restoring
Gut Health, and Optimizing Vitality.
When the body is dealing with chronic disease or low-level
systemic inflammation, the immune system becomes dysregulated. It becomes
imbalanced, and clogged with old white blood cells that aren’t functioning
well.
In this situation, boosting the immune system—a very
popular trend these days– may not be the best strategy for restoring health. The
use of “immune boosting” supplements to amplify certain aspects of an immune
system that is already imbalanced and over-extended will only perpetuate the
dysfunction.
Rather than “boosting” the system, a better goal is to
reset and rejuvenate it, and to replace worn-out immune cells with new ones to
improve immune resilience.
Fasting & Autophagy
Fasting is a well-known method for stimulating the removal
of old immune cells, producing new ones, and resetting the immune system. Fasting
triggers the process called autophagy—a break down and removal of damaged or
dysfunctional white blood cells, including those misdirected against the body’s
own tissue (autoimmunity).
Autophagy is particularly effective in destroying
immunosenescent cells which are responsible for the alteration of immune
functions due to aging.
Intermittent fasting—a meal schedule that alternates
between normal eating patterns and brief but frequent full fasts (or restricted
caloric intake)—is an effective method for increasing the rate of
autophagy. There are several different
approaches to this, including alternate-day fasting and daily time-restricted
eating.
Regardless of the method chosen, the principle is similar:
during periods of calorie restriction, the body removes senescent leukocytes and
replace them with newly generated cells, which in turn reduces the overall amount
of inflammation in the body.
Eating again following a brief fast will stimulate stem
cells to generate new leukocytes, a discovery for which Japanese cell
biologist, Yoshinori Ohsumi, won the 2016 Nobel Prize in physiology or medicine.
Within cells, a similar process of removal and replacement
occurs with the mitochondria. At that level, fasting triggers a different type
of autophagy called mitophagy, where old, damaged, dysfunctional mitochondria
are broken down and removed, allowing the remaining mitochondria to function
better. At the same time, mitophagy helps reduce the production of undesirable
inflammatory cytokines from the cell.
Intermittent fasting can take several forms, and it is a
matter of personal preference which one works best for a given. Some people
follow alternate-day fasting, a cycle of fasting on one day, and eating normally
on the next. Others prefer the “5:2 Diet,” with five days per week of
unrestricted eating and two non-consecutive days in which one eats only one
meal, restricted to 500 to 700 calories.
The “5:2 Diet” is one of several popular approaches to intermittent fasting (Image: Nuan Tang/ Shutterstock)
Still others prefer variations on time-restricted eating,
where one limits one’s eating to a relatively short daytime window, after
fasting for at least 12 hours overnight. The fasting-mimicking diet, pioneered
by Valter Longo, Ph.D., is a periodic, multi-day diet that restricts calories
but is high in unsaturated fats.
For many people, intermittent fasting is most easily
accomplished by avoiding caloric consumption for at least 12 hours (preferably
for 14 to 16 hours) after the evening meal. In my experience, aiming for a
14:10 eating pattern works well for many people. This means fasting for 14
hours between the evening meal and the first meal the next day.
It’s OK to drink unsweetened clear liquids such as water,
tea, herbal tea, and coffee while fasting. During the 10-hour eating windows, I
advise my patients to follow a health-oriented, plant-forward diet.
Daily intermittent fasting like this enhances mitophagy and
improves mitochondrial function. The mechanisms behind this are still being
explored. We know, however, that the process involves several transcription
factors that promote mitochondrial biogenesis. One example is nuclear factor 2
(NRF2), which regulates mitochondrial production of reactive oxygen species.
Fasting may enhance the production of NRF2 and improve the expression of
antioxidant regulatory genes.
A Role for Spermidine
The value of intermittent
fasting for immune rejuvenation through autophagy may be enhanced by supplementing with spermidine–a
polyamine that induces autophagy through the TOR kinase pathway. Spermidine mimics the action of caloric restriction on
the body.
While not a substitute for intermittent fasting, spermidine
supplements are particularly valuable for maintaining the rejuvenation effect during times when fasting periods must be
shorter than usual.
Improving Metabolism
Robert G. Silverman, DC, DACBN, DCBCN
The benefits of intermittent fasting for rejuvenating the
immune system and improving mitochondrial function are clear. In addition, it
also reduces inflammation and improves insulin sensitivity. Many people find that
intermittent fasting helps them lose weight by losing body fat, not muscle.
The reality is, most Americans eat half or more of their
daily calories by snacking on low-nutrient processed foods (aka junk food)
after dinner. I strongly advise patients to avoid this damaging eating pattern
by fasting for 14 hours or longer.
In refraining from adding to their blood sugar during the
fasting period, people can activate their bodies’ ability to use existing blood
sugar for energy, so there’s little left over to be stored as fat. In some
cases, the body will dip into its hepatic glycogen reserve overnight.
Being overweight or obese strains the immune system by
causing inflammation. Intermittent fasting helps with weight loss, which in
turn helps relieve the stress on the immune system and makes rejuvenation even
more effective. It’s a virtuous circle that can greatly improve immune health.
Critical Nutrients for Immunity
A well-balanced diet that emphasizes plants, high-quality
protein, and good fats, will lay the macronutrient foundation for strong
immunity. But even with a good basic diet, many people run low on some
essential minerals, particularly if they’re battling a chronic illness or
long-term inflammation.
High levels of critical nutrients are essential for
maintaining a healthy immune system and rejuvenating it through fasting. Good
nutrition is also essential for efficiently producing ATP within the
mitochondria. B vitamins, iron, magnesium, selenium, and zinc are all crucial for
peak immunity.
B Vitamins: The B vitamins
thiamine, riboflavin, and niacin are essential, as is the closely related
alpha-lipoic acid, along with amino acids such as carnitine, cysteine, and
coenzyme Q10 (ubiquinone or CoQ10).
Iron is crucial for an effective
immune system. Low serum iron is a common response to infection. It’s the
body’s way of slowing the progress of the infection by keeping microbes from
accessing the iron they need to reproduce and spread.
But immune system cells need iron to support their
metabolism. When iron is scarce, the mitochondria in immune cells can’t
generate enough energy. They become less effective at fighting infection and
generating immune memory to fight future infections.
Iron deficiency is one of the most common micronutrient deficiencies
worldwide, particularly among pregnant women, the elderly, and hospitalized
patients. Iron supplements can raise low serum iron levels and help maintain a
healthy balance between enough iron to support immune system cells while also
limiting the iron supply to pathogens.
Magnesium is essential for
hundreds of enzymatic processes in the body. In the immune system, it is vital
for forming many coenzymes and cofactors needed for the complex signaling
within and among white blood cells, and for developing antibodies.
Most Americans are magnesium-deficient. Low magnesium can
contribute to development of a cytokine storm, a severe immune reaction to an infection
in which the body releases too many cytokines into the blood too quickly, and may
also contribute to autoimmunity.
Magnesium is also needed to produce the enzymes that
metabolize vitamin D. Consequently, magnesium deficiency will reduce the
effectiveness of the vitamin D supplements someone may be taking.
Selenium is an essential micronutrient
that has a crucial role in optimal immune responsiveness. It is a potent
antioxidant that helps lower oxidative stress and reduce inflammation,
ultimately enhancing immunity. Selenium deficiency leads to less robust immune
responses to viruses and bacteria.
Zinc: Although zinc is considered
a trace mineral for dietary purposes, large quantities are essential for the
immune system. Some researchers even call it the gatekeeper of immune function,
given its importance in cytokine signaling and for mobilizing the cells of the
adaptive immune system. Low zinc levels are known to increase susceptibility to
viral infection.
Zinc is necessary for maintaining the integrity of the
pulmonary and intestinal mucosal barriers. It’s also essential for proper
function of the pathways that trigger T cell and B cell proliferation in
response to infection.
As a co-factor for many enzymes involved in immune cell
function, zinc also plays a role in balancing pro- and anti-inflammatory immune
processes.
END
Robert G. Silverman, DC, DACBN, DCBCN, is a chiropractic doctor, clinical nutritionist, national/international speaker, and author of Amazon’s #1 bestseller Inside-Out Health. He is the founder and CEO of Westchester Integrative Health Center. Dr. Silverman graduated magna cum laude from the University of Bridgeport College of Chiropractic, and also holds a Master of Science in human nutrition. The ACA Sports Council named Dr. Silverman “Sports Chiropractor of the Year” in 2015. He is on the advisory board for the Functional Medicine University, and is a seasoned health and wellness expert on the conference circuit. He is a frequently published author in peer-reviewed journals and other mainstream publications. His new book, Immune Reboot: Your Guide to Maximizing Immunity, Restoring Gut Health, and Optimizing Vitality, was released in December 2022.
Graphic representation of the relationship between zinc deficiency, Crohn’s Disease and Ulcerative Colitis (from Zupo R, et al. Nutrients. 2022)
One
in every two people with irritable bowel disease (IBD) is zinc-deficient,
according to a recent systematic review of nine studies representing more than
2,400 IBD patients.
The
prevalence of zinc deficiency, based on serum zinc measurements, was higher
among those with Crohn’s disease (CD), affecting 54% of the patients in this
subgroup, versus 41% of those with ulcerative colitis (UC).
“This
is the first meta-analytic study to be conducted on the prevalence of zinc
deficiency in IBD,” wrote lead author Roberta Zupo, at the Saverio de Bellis
National Institute of Gastroenterology, Castellana Grotte, Italy. “The present
research highlights the importance of considering zinc as a micronutrient to be
monitored, because every second IBD patient shows a deficiency.”
Zupo
and colleagues screened 152 studies that included data on nutrient deficiencies
in IBD patients. Only nine trials had sufficient data on zinc, and met the
researchers’ strict inclusion criteria. The nine studies analyzed were all
published between 2017 and 2022.
Roberta Zupo, Unit of Data Sciences, Saverio de Bellis National Institute of Gastroenterology, Castellana Grotte, Italy
The
studies represented populations from Asia, Europe, and the US. A total of 1,677
of the 2,413 pooled IBD patients (69.5%) had CD, while 736 had UC.
There
were some differences across the nine studies regarding the threshold used to define
“deficiency.” Some investigators used a cut-off of 70 μg/dL, while others defined deficiency as serum values under
10.7 μmol/L. The largest of the trials—a 996 patient
study published by Shivi Siva and colleagues at the University of Chicago
in 2017, used a threshold of 0.66 mg/mL.
But
overall there was little heterogeneity between the studies they analyzed, and the
risk of bias was low, according to Zupo.
“Zinc deficiency may predispose to growth retardation in young populations, and to loss of appetite, impaired immune function, and structural impairment of the intestinal endothelium. In severe cases, it may also drive hair loss, diarrhea, delayed sexual maturation, impotence, hypogonadism in males, and eye and skin lesions.”
Roberta Zupo, Saverio de Bellis National Institute of Gastroenterology, Castellana Grotte, Italy
Taking
the 2,413 pooled patients as a group, the overall prevalence of zinc deficiency
was exactly 50%, though this number ranged from roughly 21% to over 60% across
the nine studies. That 50% figure is substantially higher than the 15%
prevalence reported in an earlier, smaller study of this subject (Vagianos K, et al. J
Parenter Enteral Nutr. 2007).
With
two exceptions, most of the studies under review showed a pattern of higher
prevalence of zinc deficiency among the subjects with CD compared with those
who had UC. Again, there were variations between the studies in terms of the
number of CD patients who showed zinc deficiency. Two studies reporting numbers
over 80% in this subgroup.
Zupo
and colleagues believe the higher prevalence among CD versus UC patients makes
sense given what is known about the process of dietary zinc absorption.
This
trace mineral is primarily absorbed in the distal duodenum and proximal
jejunum. CD can affect any part of the GI tract, including the stomach,
duodenum, and small intestines, whereas UC typically affects only the colon and
the rectum. Consequently, CD is more likely than UC to affect the areas of the
gut mucosa involved in zinc absorption.
The
authors suggest that the zinc deficiencies observed in patients with IBD
reflect a combination of malabsorption intrinsic to this disease, and also to low
consumption of zinc-rich foods such as beans, nuts, shellfish (especially
oysters), whole grains, and dairy. Loss of zinc due to diarrhea, high-exit
fistulas, and ostomies—all of which are common in the context of IBD—also play
a role.
A
Pattern of Malabsorption
The
high prevalence of zinc deficiency fits an overall pattern of nutrient
deficiency, and even malnutrition, in IBD patients.
According
to a recent study by Stephanie Gold and colleagues at the Icahn School of
Medicine, Mount Sinai Medical Center, New York, NY, 36% of a cohort of 182
recently diagnosed IBD patients met criteria for malnutrition. The vast
majority (78%) had at least one micronutrient deficiency. Those with active
Crohn’s were 2.8 times more likely to be malnourished (Gold SL, et al. Inflamm Bowel Dis. 2022).
Chiara Vigano, MD, Division of Gastroenterology, San Gerardo Hospital
Chiara
Vigano and her team at the San Gerardo Hospital, Monza, analyzed data from 295
adults with IBD (50% CD, 50% UC) at 11 hospitals in the Lombardy region of
Italy.
They found that 23% of the patients had at least one significant micronutrient deficiency, with deficiencies in B12, folate, and ferritin being among the most prevalent.
Vigano
and colleagues did not see any statistically significant differences between
the CD and UC patients in terms of disease-related malnutrition. However, they
did see correlations between disease-associated malnutrition and higher median
levels of C-reactive protein. This suggests a relationship between poor
nutritional status and increased inflammation, though from the perspective of
causality the direction of this relationship is not clear.
They
presented
their data
as a poster at the 2022 United European Gastroenterology Week conference in
Vienna last October.
Deficiencies of zinc and other trace elements are major contributors to the symptom burden of IBD, and to the adverse impact of this disease on patients’ quality of life.
A recent study by researchers at the National Institute of
Medical Science and Nutrition in Mexico City indicates that vitamin D
deficiency is also common among IBD patients.
Andrea Sarmiento-Aguilar and colleagues reviewed medical
records from 270 IBD patients (83% UC, 17% CD), 225 of whom had vitamin D measurements
included in their charts. Of this group, 48% were vitamin D insufficient,
defined by serum levels between 21-29 ng/mL. An additional 34% were frankly
deficient, based on a cutoff of 20 ng/mL.
Major Impact on QOL
Dr. Zupo and her colleagues hold that deficiencies of zinc and
other trace elements are major contributors to the symptom burden of IBD, and to
the adverse impact of this disease on patients’ quality of life.
A key component for the proper functioning of many enzymes and
transcription factors, zinc is also important for regulating immune system
responses, cell cycling, and apoptosis.
“Zinc
deficiency may predispose to growth retardation in young populations, and to
loss of appetite, impaired immune function, and structural impairment of the
intestinal endothelium. In severe cases, it may also drive hair loss, diarrhea,
delayed sexual maturation, impotence, hypogonadism in males, and eye and skin
lesions,” says Zupo.
“All
these aspects highlight the importance of early nutritional preventive
management in IBD settings, from better quality of life and healthcare burden
perspectives.”
She
and her colleagues consider the relationship between zinc deficiency and IBD to
be bidirectional, since low serum zinc levels tend to exacerbate inflammation
and damage to the GI mucosa, and mucosal damage impedes absorption of zinc and
many other nutrients.
A
Role for Supplementation?
The
big question is whether zinc supplementation or intentionally increasing the
intake of zinc-rich foods can raise serum zinc levels in IBD patients and
mitigate the symptom burden.
That question is largely still unanswered, although there are a few studies suggesting that supplementation may be beneficial.
In
2001, Sturniolo and colleagues published a non-controlled study of 12 patients
with quiescent CD but who showed increased intestinal permeability based on measurements
of lactulose/mannitol ratios. Following eight weeks of supplementation with
zinc sulfate (110 mg thrice daily), the mean lactulose/mannitol ratios were
significantly lower, and 10 of the 12 patients were above the cutoff for “normal”
permeability (Sturniolo GC,
et al. Inflamm Bowel Dis. 2001).
In
other words, zinc supplementation seemed to tighten the loose and permeable
epithelial junctions.
Various researchers have proposed doses ranging from 40 mg/day for 10 days to up to 110 mg per day for 8 weeks in the IBD population.
Commenting
on the Sturniolo paper, Zupo and colleagues note that, “This latter finding is
critical because intestinal epithelial barrier dysfunction may allow leukocytes
to pass through, causing exposure to a “storm” of luminal antigens, a hallmark
of IBD activity.”
In their
993-patient study, Siva and her team reported on a subset of 232 CD patients
who were zinc-deficient at baseline, but who were able to normalize their serum
zinc levels via supplementation or dietary changes over a period of 12 months. Compared
with those who remained zinc-deficient, the 76 patients who were able to raise
their zinc levels into the normal range (above 0.66 mcg/ml) had fewer
hospitalizations, fewer surgeries, and fewer CD-related complications. The
differences were statistically significant.
The
University of Chicago researchers observed a similar pattern among their 174 UC
patients, although in this subgroup normalization of zinc levels did not result
in a significant decrease in subsequent surgeries (Siva S, et al. Inflamm
Bowel Dis. 2017).
These
data are promising, but they need to be corroborated by prospective
supplementation trials.
In
their 2017 review on the subject of nutrient deficiencies in IBD patients, Fayez
Ghishan and Pawel Kiela at the University of Arizona’s department of
pediatrics, note that IBD-associated diarrhea is a strong indication for zinc
supplementation (Ghishan
FK, Kiela PR. Gastroenterol Clin North Am. 2017).
They,
and other authors, have suggested that the current RDAs for zinc—11mg/day for
adult males, and 8 mg/day for females—may be too low for zinc-deficient IBD
patients. Various researchers have proposed doses ranging from 40 mg/day for 10
days to up to 110 mg per day for 8 weeks in the IBD population.
But
Ghishan and Kiela urge caution when pushing the doses. They point out that the
upper limit for avoidance of potential toxicity is 40 mg/day. Beyond that,
there’s a risk that zinc will interfere with absorption of iron and copper. On
the other hand, it is important to be aware that increased intake of calcium or
folate can impair absorption of zinc.
Also
keep in mind that citric acid may improve zinc absorption, whereas iron,
copper, dietary fiber, and phytates found in many types of legumes and seeds,
may inhibit absorption.
Based
on studies of patients with cystic fibrosis, chronic pancreatitis, or other
conditions that tend to cause micronutrient malabsorption, Zupo and colleagues
propose that daily zinc intake in the range of 30–40 mg daily, is reasonable in
IBD patients.