




The world has a drug problem. A drug pollution problem, that is.
Infiltration of potentially bioactive drug metabolites into waterways and groundwater is a widespread and growing phenomenon affecting nearly every region of the planet.
According to a recent worldwide study, active pharmaceutical ingredients (APIs) have been detected in streams and rivers on every continent, including Antarctica, sometimes in concentrations that could have physiological effects on humans.
Drug-derived pollutants enter the environment via direct release of byproducts of manufacture, as well as from animal agriculture, patient excretions into sewage and waste water, and inappropriate disposal of unused or outdated medications.
A recent report by the UK’s Centre of Expertise for Water notes that anywhere from 30% to 99% of a given dose of medication is excreted in urine or feces. This means that every day, massive quantities of APIs end up in toilets and ultimately, in waste water.
Globally, 80% of all waste water is discharged directly into streams, rivers, and waterways. And even in technologically advanced countries, waste water treatment plants (WWTPs) are generally unable to remove and neutralize most APIs. As a result, a host of diverse, potentially toxic drug compounds enter the environment.
“At the moment many people don’t think about where our medicines come from or what happens to them after we swallow them. Medicines are a vital part of our healthcare system, so we need to find ways to use them without poisoning the environment at the same time.”
–Kelly Thornber, PhD, College of Life & Environmental Sciences, University of Exeter
Environmental researchers have been calling attention to the problem for decades, but few countries are doing anything to mitigate pharmaceutical pollution.
Recently, though, the nation of Scotland took the lead in confronting this issue through multiple initiatives to better monitor the problem, raise public awareness, and shift physicians’ prescription choices.
Scotland Embraces Eco-Rx
Among the projects is a joint effort between NHS Highlands and UK Research & Innovation (UKRI) to develop “eco-directed” prescribing guidelines that integrate environmental sustainability ratings with clinical efficacy and cost data.
Within this new framework, if two drugs are comparable in safety and expected efficacy, then the decision about which to prescribe should favor the drug with the least “ecotoxicity.” The guidelines are still in early stage development, but they represent a major step forward because they will ultimately give Scottish doctors new objective tools for factoring environmental impact into their clinical decisions.
According to the Scottish National Health Service (NHS), the country’s drug prescription rates have increased by roughly 40% over the past 15 years. In the 12 months from 2018 to 2019, Scots took more than 104 million pharmaceuticals. Each year, Scotland’s total prescription drug bill reaches roughly £1.8 billion.
The guidelines project, which is supported in part by funding from the Scottish government, is part of Scotland’s broader One Heath Breakthrough Partnership (OHBP)—an interdisciplinary public health initiative based on the principle that “human health, animal health, and environmental health are closely interconnected and interdependent,” and that “water and water quality are central to this connectivity.”

Because practitioners write the prescriptions, they are the upstream regulators of the flow of pharmaceuticals into their communities. By making practitioners aware of the environmental impact of their treatment choices, OHBP’s leaders hope to reduce unnecessary or ineffective prescriptions, and to steer doctors and nurses toward the drugs with the lowest ecological risk.
Current NHS formularies in the UK, “consider patient safety, clinical effectiveness, and cost effectiveness, but they do not consider the environmental impact of a medicine,” says OHBP in a press release. Ultimately, the authors hope to translate the new guidelines into recommendations that can be implemented internationally.
An Upstream Solution

“Pharmaceutical chemicals are vital components of modern health care, but their contamination of global waterways is threatening environmental and human health, contributing to biodiversity loss, driving antimicrobial resistance, and jeopardising progress towards the sustainable development goals, wrote Kelly Thornber, of the College of Life and Environmental Sciences, at the University of Exeter, in a recent editorial in The Lancet.
Entitled First Do No Harm, the article outlines the astonishing scope of the global drug pollution problem, and challenges the inertia among policy-makers, medical practitioners, and industry stakeholders.
Within this new framework, if two drugs are comparable in safety and expected efficacy, then the decision about which to prescribe should favor the drug with the least “ecotoxicity.”
“With the global pharmaceutical market now worth more than US $1.25 trillion and continuing to grow as populations age and suffer from more chronic, non-communicable diseases, there is an urgent need to integrate pharmaceutical pollution into sustainable health-care strategies, alongside efforts to reduce carbon and plastic waste,” wrote Thornber and colleagues.
Notably, they call for, “greater prioritisation and investment into preventative health care and non-pharmaceutical treatment options.”
The concept of eco-directed sustainable prescribing (EDSP) is not new. A landmark 2014 paper by Christian Daughton outlined the core concepts, stressing that control of pharmaceutical pollution requires upstream interventions.
“Reducing API entry to the environment has relied solely on conventional end-of-pipe pollution control measures such as wastewater treatment and take-back collections of leftover, unwanted drugs (to prevent disposal by flushing to sewers),” wrote Daughton, a US Environmental Protection Agency scientist. “An exclusive focus on these conventional approaches has ignored the root sources of the problem and may have served to retard progress.”

He contends that a more effective, less costly strategy would be to promote changes in prescribing habits that minimize dose levels, reduce unnecessary prescriptions, and encouraging doctors to consider API excretion profiles when making decisions.
In 2019, occupational hazard researchers in Wuhan, China, surveyed 405 physicians at 5 government hospitals throughout the Hubei province, about their perceptions and attitudes toward API pollution and the concept of EDSP.
They found a high level of concern about API pollution, and a general willingness to participate in EDSP programs. But none of the surveyed physicians said ecological concerns influence their current prescribing decisions, and 97% said they had a “wait and see” attitude toward EDSP. Many worried that low-dose prescribing or use of more eco-friendly drugs might diminish clinical outcomes.
Rivers Full of Drugs
A recent study of water samples from 258 rivers in 104 countries on all seven continents reveals the scale of API pollution worldwide.
John Wilkinson and colleagues at the University of York, UK, working with a dedicated team of researchers all over the world, found active pharmaceutical ingredients (APIs) in all of the rivers tested.
The Wilkinson survey, published in February 2022 in PNAS, is the largest global assessment of drug pollution ever undertaken. It is remarkable not only by its scope but by its uniformity of analytical methods.
The water samples came from 1,052 sites along the 258 rivers, and the investigators assessed them for the presence of 61 known APIs. Sampling sites included populous cities such as New York, Delhi, Seoul, London, and Kinshasa, as well as small villages in areas far from any major metropolis. The survey covered a wide range of geography and topography, from alpine tundra (Colorado) to desert (Tunisia).
With the exception of samples from a Yanomani village deep in the Venezuelan Amazon where few if any people have ever taken pharmaceuticals, and from sparsely populated parts of Iceland, all other sampling sites showed at least one API in the water.
The highest mean cumulative API concentration, 70.8 µg/L, was found in water samples from Lahore, Pakistan. One site in that city had a maximum cumulative concentration of 189 µg/L. La Paz, Bolivia was next, with a mean of 68.9 µg/L, and a maximum of 297 µg/L. Addis Ababa, Ethiopia was third, with a mean of 51.3 µg/L, and a maximum of 74.2 µg/L.
A cumulative API level above 15 µg/L puts a sampling site in the 90th percentile for total drug pollution.
Several US cities were above the 70th percentile: Dallas showed a mean cumulative API concentration of 10 µg/L, and Las Vegas showed a cumulative concentration of 5 µg/L.
In Europe, the most polluted samples came from Madrid, with a cumulative mean of 17.1 µg/L, followed by Sofia, Bulgaria, with a mean of 12 µg/L.
With the exception of samples from a Yanomani village deep in the Venezuelan Amazon where few if any people have ever taken pharmaceuticals, and from sparsely populated parts of Iceland, all other sampling sites showed at least one API in the water.
Not surprisingly, caffeine and nicotine were among the most frequently identified APIs, found in almost all water samples in all countries. Acetaminophen (paracetamol) was also nearly ubiquitous.
There were also 14 APIs commonly found in rivers from all continents except Antarctica: atenolol (β-blocker), carbamazepine (antiepileptic), cetirizine (antihistamine), citalopram (antidepressant), desvenlafaxine (antidepressant), fexofenadine (antihistamine), gabapentin (anticonvulsant), lidocaine (anesthetic), metformin (antihyperglycemic), naproxen (anti-inflammatory), sitagliptin (antihyperglycemic), temazepam (benzodiazepine for insomnia treatment), trimethoprim (antimicrobial), and venlafaxine (antidepressant).
Carbamazepine was found in 62% of all river catchments, and metformin was identified in over 50% of all the sampling sites worldwide.
Marked Regional Variations
Worldwide, the APIs found at the highest concentrations were paracetamol, caffeine, metformin, fexofenadine, sulfamethoxazole, metronidazole, and gabapentin. But there were marked variations in the types and quantities of drugs found in different countries. This reflects differences in disease prevalence, disparities in access to drugs, differences in the presence of drug manufacturing plants, and disparities in waste water treatment capacity.

“Socioeconomic drivers may, in part, help explain the environmental distribution of APIs,” wrote Wilkinson and colleagues. “In this study, concentrations of APIs were found to be highest in countries of lower-middle income (gross national income [GNI]-index: 995 to 3,895 USD$) than in countries of any other income classification reported by the World Bank.”
Wilkinson hypothesizes that this pattern results from the fact that people in lower-middle income countries typically have greater access to prescription drugs than do those in low income countries, but in the middle-income countries, waste water treatment is not as advanced as it is in high-income countries.
“Upper-middle and high-income countries, while having access to medicines, typically have higher connectivity to waste water treatment, more sophisticated waste management systems, and tighter regulation of medicinal use, thus resulting in relatively lower environmental API concentrations.”
As Kelly Thornber and colleagues point out in their Lancet article, while drug consumption is highest in upper-income nations, drug production is largely based in low-to-middle income countries, which tend to have the heaviest burden of manufacture-related pollution. Thornber adds that there is also a long history of high-income countries sending unused meds nearing expiry dates to low-income countries, “potentially leaving them with large stocks of out-of-date medicines without safe disposal options.”
A Real Threat?
Are waterborne APIs really a threat to human health? It’s a difficult question to answer, because it’s a difficult question to study.
There are many inherent challenges in proving causality between a specific environmental variable and a particular disease. In the context of pharmaceutical water pollution, there are myriad bioactive metabolites, with many potential effects, present at relatively small concentrations that vary from place to place.
As with other environmental issues, there are few private sector financial incentives to study this question, and government funding streams are limited.
But there’s reason to believe API pollution could pose a significant human risk. Numerous animal studies show that environmental exposure to APIs has deleterious effects including:
- Fluoxetine-induced developmental delays in frog tadpoles (Foster HR, et al. Environ Toxicol. 2010)
- Oxazepam-induced changes in salmon migration behavior (Hellstrom G, et al. Nature Comm. 2016)
- Multigenerational ethynyl estradiol-induced reproductive failure in zebrafish (Nash JP, et al. Environ Health Perspect. 2004)
- Alterations in crayfish feeding behavior and metabolism by citalopram (Reisinger AJ, et al. Freshwater Ecol. 2021)
- Increases in prevalence of intersex fish (genetically male but with immature ova in their testes) linked to estrogenic compounds in Chesapeake Bay waters (US Geological Survey). In one study of 19 National Wildlife Refuges, over 60% of smallmouth bass captured showed intersex characteristics, associated with increased presence of estrogenic compounds in the water (Iwanowicz LR, et al. Ecotoxicol Environ Saf. 2016).
These are just a few of the many reports indicating that environmental APIs can alter animal physiology and behavior. And that’s on top of the effect of excreted antibiotics in promoting microbial resistance (Glebultowicz J, et al. Molecules, 2020).
Waterborne APIs don’t just stay in the water; they bioconcentrate up the food chain.
Scientists from the Cary Institute of Ecosystem Studies, in collaboration with researchers at Monash University, Melbourne, traced the presence of 69 waterborne APIs in filter-feeding aquatic insect nymphs that become flying adults, which are then eaten by land-dwelling spiders, birds, and bats.

“Platypus eat aquatic insects. If we scale up our findings, a platypus living in a creek receiving treated wastewater effluent could receive the equivalent of half of a recommended human dose of antidepressants every day. This intake is likely to have biological effects,” says Cary Institute ecologist, Emma Rosi, PhD.
This should not be surprising. “APIs are biologically active molecules, specifically designed to interact with biochemical pathways, of which many are conserved in both aquatic and terrestrial organisms,” writes John Wilkinson, author of the global rivers study.
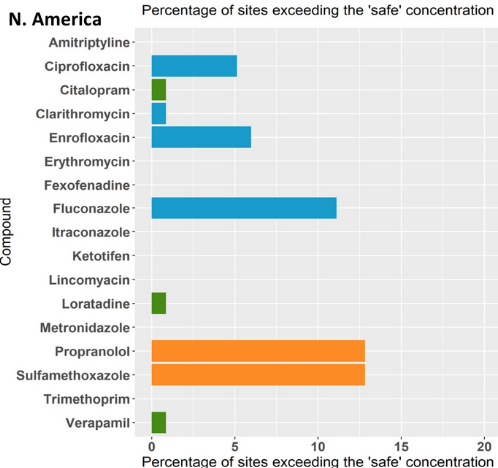
Most APIs detected in the world’s rivers were found at levels below their predicted no-effect concentrations (PNECs). The PNEC for a given drug is the threshold below which the compound in question is not likely to have biological impact on humans. However, 26% of the 1,052 study sites reported finding at least one API that exceeded its PNEC.
These were: sulfamethoxazole (antimicrobial), propranolol (β-blocker), loratadine (antihistamine), amitriptyline (antidepressant), citalopram(antidepressant), fexofenadine (antihistamine), verapamil (Cachannel blocker), and ketotifen (antihistamine), all of which were found at levels above PNEC somewhere in the world.
Wilkinson points out that the sub-PNEC levels of many drugs gives a false sense of security regarding risk, because PNECs do not account for the long-term impact of ongoing exposure to multiple randomly mixed bioactive compounds.
“The highest number of APIs detected at a single site was 34 at a location in the Kai Tak River in Hong Kong. Ecological risks, therefore, could well be greater than predicted for the single APIs due to toxicological interactions of these mixtures.”
An Accelerating Problem
Without strong and coordinated preventive action, pharmaceutical pollution will only get worse in the future as populations age, chronic diseases increase, and drugs become more widely available in low-income nations.
“Lipophilic compounds, such as steroid hormones, have tendency to accumulate in tissues and may cause undesirable effects after accumulation in the long term. Populations with inadequately developed or compromised liver and kidney functions….are at high risk of drug bioaccumulation due to poor biological clearance.”
–Pakoyo Fadhiru Kamba, Dept. of Pharmacy, Makerere University, Kampala, Uganda
There are currently over 21,000 prescription pharmaceuticals in use across the globe, creating a global market now worth more than $1.25 trillion. That will only grow in the years to come.
“The global consumption of drugs for acute conditions has significantly increased over the years. A recent study of antibiotics consumption in 71 countries representative of all the world’s geographic and economic diversity shows that it increased 36% from 54.1 billion standard dosage units (tablets, capsules, ampoules, vials) to 73.6 billion units over the ten-year period 2000-2010” writes Pakoyo Fadhiru Kamba, of the department of pharmacy at Makerere University, Kampala, Uganda.
In their excellent review of the global API pollution problem, Kamba and colleagues stress that drug consumption is soaring in lower income developing countries.

They point out the widespread problem of subtherapeutic dosing, which can raise personal and environmental risks without even delivering the expected clinical benefit. This can occur because of poor adherence or deliberate rationing of expensive meds.
“Lipophilic compounds, such as steroid hormones, have tendency to accumulate in tissues and may cause undesirable effects after accumulation in the long term. Populations with inadequately developed or compromised liver and kidney functions, namely, the newborns, infants below two months, prematures, the elderly, and all those with hepatic and renal disorders are at high risk of drug bioaccumulation due to poor biological clearance,” Dr. Kamba states.
Widespread Indifference
The Ugandan authors call out global indifference toward the problem of pharmaceutical pollutants, noting that the US, the UK, and the European Union have no regulations on drug levels in waterways or groundwater.
“Central to the indifference is the notion that at the subtherapeutic concentrations at which many pharmaceuticals are present in the environment, their biological effects are insignificant,” they write. “However, reliance on acute studies ignores the delayed effects for those drugs which bioaccumulate. Additionally, they ignore the potential adverse impact of additive, potentiation and synergistic interactions from simultaneous contamination with multiple pharmaceuticals.”
Given the daunting scale of the drug pollution problem, Scotland’s new eco-prescribing initiative may seem like a small step. But it is a bold move in the right direction, one that will hopefully influence similar policy decisions in other countries.
As Exeter’s Kelly Thornber stated in a press release accompanying her recent Lancet article, “At the moment many people don’t think about where our medicines come from or what happens to them after we swallow them. Medicines are a vital part of our healthcare system, so we need to find ways to use them without poisoning the environment at the same time.”
She adds, “Human healthcare should not come at such a high environmental cost.”
END


