The Coronavirus epidemic has wrought major changes on the medical landscape. If you’re struggling to figure out how to continue caring for your patients in this time of social distancing, don’t worry. You are definitely not alone.
this time of social distancing, don’t worry. You are definitely not alone.
It can be distressing to close the clinic doors and rely solely on technology to treat patients. If you have never utilized telemedicine or phone visits it is doubly challenging to abruptly refashion your entire practice.
But with quarantine and social distancing in effect in most states now, and no definitive end date, it is important to quickly and efficiently transition your practice into a virtual one. Telemedicine can be a life-saver, not only for your patients but for the future of your clinic.
At Snow Creek Medicine in Anchorage, Alaska, we have a lot of experience using technology to treat patients in rural areas where obtaining healthcare can be challenging. Streamlining the billing is crucial for making this work.
As a deluge of patients concerned about their COVID-19 exposure demand your attention, on top of all the routine medical issues you’re already handling, you need to assure that you and your staff are up to date on federal and state telemedicine guidelines, which are changing quickly these days.
Being knowledgeable about these things will help ease your patients’ fears about being able to access their own physicians in times of need.
Thankfully HIPAA and billing regulations are being relaxed all over the US to allow physicians and their staff-members to transition more easily into the burgeoning world of electronic medicine.
Telemedicine vs Virtual Check-In
According to the American Medical Association, a telemedicine visit is defined as an online remote consultation that utilizes any or all of the following:
- Real-time, audio-video communication tools (telehealth) that connect physicians and patients in different locations.
- Store-and-forward technologies that collect images and data to be transmitted and interpreted later.
- Remote patient-monitoring tools such as blood pressure monitors, Bluetooth-enabled digital scales and other wearable devices that can communicate biometric data for review (which may involve the use of mHealth apps)
- Verbal/Audio-only and virtual check-ins via patient portals, messaging technologies, etc.
A full telemedicine visit using real-time video can be billed the same way as an in-person office visit.
This is different from a phone-based virtual check-in call, which is, “a brief conversation that mitigates the need for an in-person visit.” Those are also billable, provided they meet certain criteria, but they are different from a full telemedicine visit.
The regulations stipulate that new patients are to be seen by telemedicine only, not treated via phone contact or text messaging alone. Established patients can make use of these other electronic visit types in addition to telemedicine.
In addition to physicians, other Qualified Health Professionals (QHPs) are able to bill for phone visits and for virtual check-ins, according to the AMA guidelines.
The AMA distinguishes a QHP as, “an individual who is qualified by education, training, licensure/regulation (when applicable), and facility privileging (when applicable), who performs a professional service within his/her scope of practice and independently reports that professional service.”
The list of QHPs includes those who cannot bill E/M codes independently. The list of possible QHPs includes certified nurse specialists (CNS), physician assistants (PA), certified nurse midwife (CNM), physical therapists (PT), and the like.
Telemedicine & COVID
With the outbreak of COVID-19, all payers including Medicare are now covering telemedicine services. Further, each state has mandates for what it expects payers to cover under all plans, regardless of the individual patients’ deductible levels.
Billable telemedicine visits must be synchronous, which means they include real-time audio and visual communication. Until COVID, the HIPAA laws were fairly strict about which communication platforms could be used for billable remote visits. Currently, those rules are being relaxed to allow nearly any manner of synchronous communication.
Free services like FaceTime, WhatsApp, and Facebook are good stopgaps for practices just getting started with telemedicine that did not have dedicated telehealth platforms in place prior to the pandemic.
Many EHR programs have built in functions to allow HIPAA secure communication, and this would be preferable to the less-secure options listed above.
Other sites such as Updox and Doxy offer free or very affordable, synchronous, HIPAA-secure telemedicine solutions.
Billing for telemedicine visits is simple. With any usual E/M code you would use for an in-person office visit, simply add the modifier -95 to denote Telemedicine Services. The Place of Service (POS) should be coded as 02, Telehealth. For example: 99214.95 POS 02.
Phone Visits & “Store and Forward”
Patients often have questions that may not require an entire visit, but do require some attention. These brief conversations can be related to medications, further questions regarding a previous treatment plan, or a new condition that does not require a full in-person visit. This is true both for COVID-19 concerns, and for routine medical issues.
 To be billable, these phone-based services must be patient-initiated. In other words, you cannot bill for appointment reminders or medication refills.
To be billable, these phone-based services must be patient-initiated. In other words, you cannot bill for appointment reminders or medication refills.
Again, keep in mind the AMA distinction that these brief check-ins and phone calls “mitigate the need for an in-person visit.” These calls may include triaging your patients to local labs or hospitals to diagnose and treat for possible COVID-19.
Most states are also allowing for asynchronous or “store and forward” transfers which permit patients and physicians to transmit medical images or information without an actual phone visits. These asynchronous transmissions can include email, text
messages, portal messages, Facebook messages, etc.
Keep in mind that in order to document appropriately, these transmissions need to be saved in the patient record.
There’s some variation in how different payers are handling these Store and Forward transactions. You’ll need to contact your specific payers to see how they are managing these types of interactions, as it may vary.
Coding for COVID-19
Over the next several months many patients will be concerned about possible or actual exposure to the coronavirus. In order for the cost-shares to be waived for diagnosis of COVID, it is vital that you use the appropriate diagnosis codes.
The AMA has created a new code for those who have been tested and confirmed to have COVID-19, U07.1, COVID-19, virus identified.
This code became effective April 1, 2020.
Note that COVID-19 cannot be diagnosed via telemedicine. The code U07.1 is only to be utilized for those patients whose tests came back positive for coronavirus.
For patients that have not been tested for COVID, and for whom the U07.1 code cannot be applied, the CDC and AMA have instructed us to code the resulting condition(s).
For example, a patient presenting with pneumonia due to the coronavirus is to be coded with primary J12.89, other viral pneumonia, with a secondary code of B97.29, Other coronavirus as the cause of diseases classified elsewhere. B97.29 is only to be used as a secondary code to another condition, and is not to be used with a patient with suspected COVID-19
For patients who are concerned with possible exposure, but have not had a confirmatory test, it is appropriate to use code Z03.818, Encounter for observation for suspected exposure to other biological agents ruled out.
For those who have had actual exposure to people definitively diagnosed with COVID-19, the Z20.828, Contact with and (suspected) exposure to other viral communicable diseases code would be appropriate.
For patients presenting with signs and symptoms, but who do not have a definitive diagnosis or confirmed exposure, assign a code for each sign and symptom such as R05 Cough, R06.02 Shortness of breath, R50.9 Fever unspecified, etc.
The Centers for Disease Control and Prevention (CDC) has provided a supplemental Official Coding Guidelines handout, available on the agency’s website.
The AMA has done a fantastic job pulling all this information together in a packet, creating several scenarios on how to code, whether it’s for a COVID-19 or non COVID-19 patient. You’ll also find general guidelines on everything outlined above.
Beyond the national guidelines, it is also vital to understand your own state’s mandates and how that will translate cost to your patients.
Other Considerations
Be sure to contact your malpractice insurance carrier about your inclusion telehealth in your practice, and make sure it is covered.
The coding guidelines and telemedicine advisories can change daily these days, so keep up to date with information directly from the CDC and AMA. Also follow your state’s mandates closely to avoid patient confusion.
This article is not meant to be a catch-all solution set, as each medical practice is unique, and the state and federal regulations about coding and telemedicine are in constant flux.
But this information can serve you as a starting point for establishing and streamlining your remote practice whether you are seeing COVID-19 or non COVID-19 patients.
Telemedicine was rising before the coronavirus epidemic. It is a vital tool in the current conditions of quarantine and social isolation, and it will only continue to grow in the aftermath of COVID. If you understand how to utilize and code for it optimally, it will help your practice thrive.
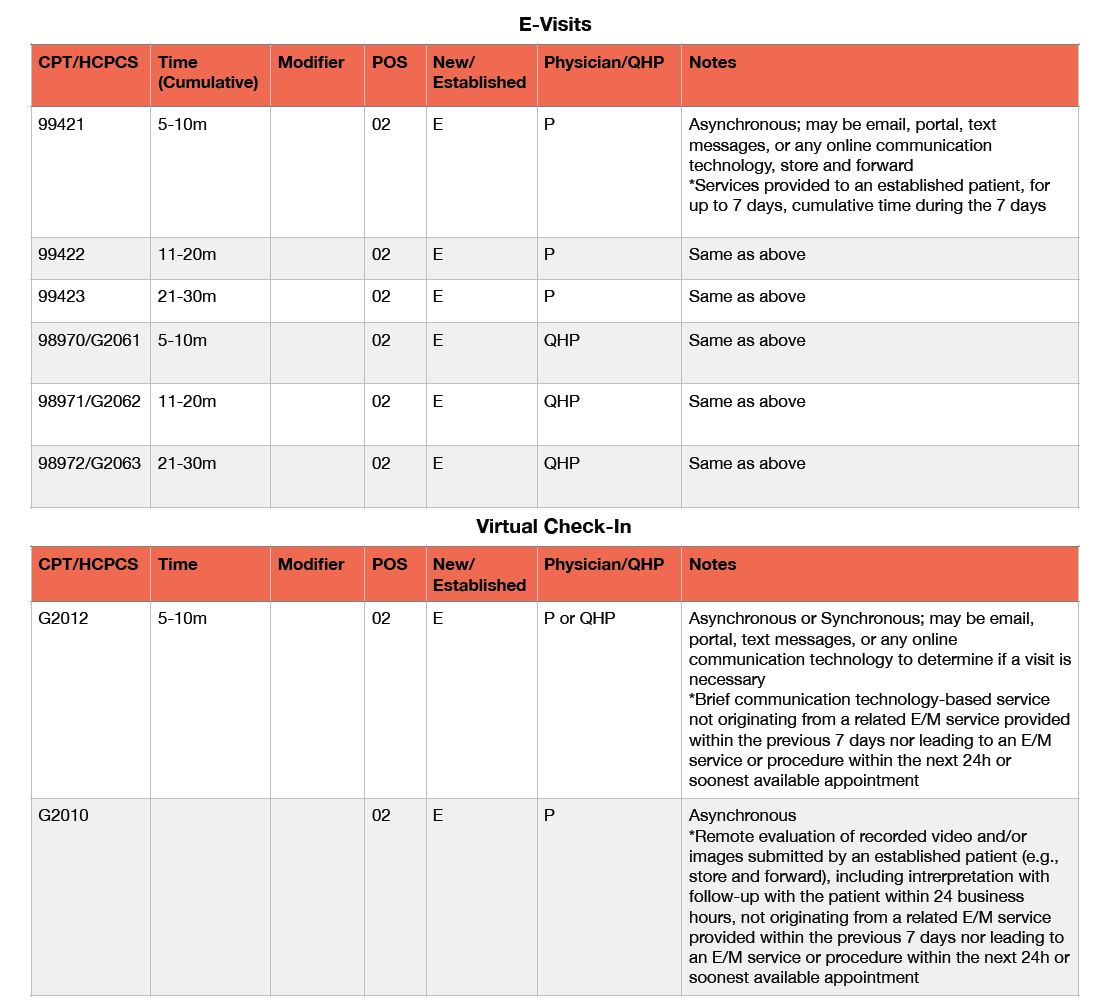
The following charts, pulled directly from the CDC and AMA, are a helpful resource.
Thank you all for your efforts in taking care of your patients during this age of rapidly changing tides.
Stacy Collier is the practice manager and billing specialist at Snow Creek Medicine, the clinic of Allison Kelliher, MD, in Anchorage, AK. In additition to her management role, Stacy also assists Dr. Kelliher in Corrective Exercise Therapy. She is a certified personal trainer with a special focus on helping people living with low back, shoulder, hip, and knee pain.