




Loss of olfaction is one of the most common and vexing sequelae of Covid-19, often persisting for many months after the acute phase of the infection.
The vast majority of Covid patients experience some degree of olfactory impairment, and roughly one quarter fully lose the sense of smell (anosmia) during the acute phase of the infection (Moein ST, et al. Int Forum Allergy Rhinol. 2020). One estimate suggests that in 45% of all Covid cases, anosmia and the related problem of ageusia (loss of taste) are the only symptoms of the infection.
For most, this loss of the “chemical senses” is transient, clearing up within a few weeks. But for a significant number—the best estimates are in the range of 18-30%–the problem persists for months, even years (Lechien JR, et al. J Int Med. 2022. Paranhos ACM, et al. JAMA Network Open. 2022). Statistically, persistent olfactory disruption correlates with severity of the initial acute phase of Covid. Age is also a risk factor.
“There are several possibilities for the causation of COVID-19-induced anosmia. One is damage to the morphology of the olfactory epithelium, where the olfactory sensory neurons reside. The second possibility is damage to the morphology of the olfactory bulb, which will obstruct signal transfer to the brain. The third possibility is the inflammatory immune response, which can weaken the olfactory system,” explained Sakicho Koyama, PhD, a neuroscientist at Indiana University, Bloomington, who studies olfaction.
Given the vast number of Covid cases worldwide, there are many thousands of people now living with blunted senses of smell and taste. So far, there are no drug therapies or surgical procedures that effectively reverse anosmia. Though several studies suggest that oral corticosteroids can help, they are by no means curative.
What can be done?

According to Dr. Koyama and an interdisciplinary research team based at universities in the US and Japan, olfactory training—the use of phytochemical-rich essential oils—holds great potential for helping people restore their sense of smell after Covid.
Last year, the group published a comprehensive review detailing the physiology of olfaction, the ways in which it is damaged by respiratory viruses, and the mechanisms by which olfactory training addresses the problem (Koyama S, et al. Int J Mol Sci. 2021).
The vast majority of Covid patients experience some degree of olfactory impairment, and roughly one quarter fully lose the sense of smell (anosmia) during the acute phase of the infection
Though not widely known, olfactory training has been used to successfully treat anosmia caused by other types of viral infections. Dr. Koyama’s team, and several others, contend that it can be equally effective in the context of long Covid.
Promoting Regeneration
Olfactory training, also called smell training, involves deeply sniffing specific plant-derived essential oils two or more times daily for several months. This is typically after baseline assessment of olfactory loss using a method such as the University of Pennsylvania Smell Identification Test (UPSIT) or the Sniffin’ Sticks test.
Damaged olfactory neuroepithelium can regenerate. As in other epithelial linings, the basal cells underlying the olfactory epithelium undergo continuous division and cell replacement. Likewise, the olfactory bulb also receives a constant influx of progenitor cells, which differentiate into granule cells that then integrate with neurons, mitral cells, and tufted cells.
A diverse range of plant-derived compounds appear to stimulate these regenerative processes.
“Essential oils, including the oils used in smell training (rose, lemon, clove, eucalyptus), contain several hundred chemical constituents. If the bioactive properties in these oils are involved in such improvements, selection of oils based on the bioactive properties of the chemical constituents may produce better improvements,” Koyama wrote adding that she and her colleagues hope their paper will serve, “as a road sign to guide much needed studies with a perspective on the bioactive properties of phytochemicals.”
Henning & the Odor Prism
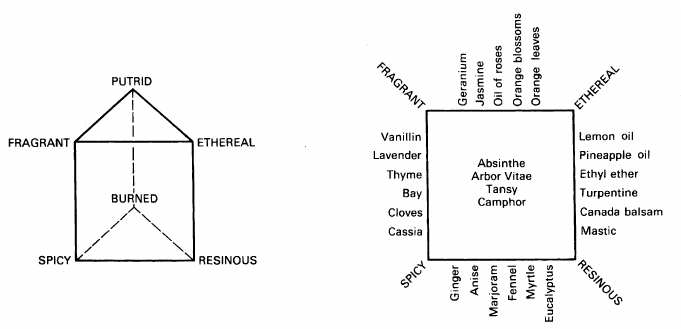
Olfactory training began with Hans Henning, an early 20th Century German psychologist who attempted to systematically categorize the myriad scents to which humans are sensitive. Henning’s “Odor Prism,” first published in 1916, is a model roughly analogous to the color pyramid, that defines six primary odor categories, translated from German as: Flowery, Putrid, Ethereal (Fruity), Spicy, Burnt, and Resinous (Henning, H. (1916) Der Geruch. Barth, Leipzig).
Between each of these six “cardinal” scent qualities, there is a continuum or spectrum. Based on the available knowledge of chemistry in his day, Henning tried to identify specific chemical constituents that give particular substances their unique aromas, and to place them along the spectra between the six key categories.
In the US, Henning found an early champion in Malcolm MacDonald, a University of Pennsylvania psychologist, who wrote: “Henning has a chemical theory of the olfactory stimulus which, if it held rigorously would be a valuable aid in determining the stimuli for the different regions of the prism.” (MacDonald M. Am J Psychol. 1922). Though his own work pointed to gaps in Henning’s model, MacDonald saw the Odor Prism as “an advance, a first approximation to the truth.”
Researchers today understand vastly more about olfaction and phytochemistry than did Henning and his generation. But some of Henning’s core concepts have been validated by modern research. The four most commonly used essential oils for olfactory training—rose, lemon/citronella, cloves, and eucalyptus—became standards because they represent four of Henning’s six key categories (flowery, fruity, spicy, and resinous).
Clinical Impact
In 2009, Thomas Hummel and colleagues at the Smell & Taste Clinic, University of Dresden Medical School, published a landmark study of 56 patients with persistent sensorineural olfactory loss. In some cases, the impairment was caused by direct trauma. In others it followed an upper respiratory viral infection, or was deemed “idiopathic.” Forty of the 56 undertook olfactory training using rose, eucalyptol, citronella and eugenol (clove), twice daily for 12 weeks. The other 16 patients did not have any form of therapy.
Damaged olfactory neuroepithelium can regenerate. As in other epithelial linings, the basal cells underlying the olfactory epithelium undergo continuous division and cell replacement. A diverse range of plant-derived compounds appear to stimulate these regenerative processes.
“Compared to baseline, training patients experienced an increase in their olfactory function, which was observed for the Sniffin’ Sticks test score and for thresholds for the odors used in the training process. In contrast, olfactory function was unchanged in patients who did not perform olfactory training.” (Hummel T, et al. Laryngoscope. 2009).
In 2018, Janine Gellrich in Dr. Hummel’s lab in Dresden used magnetic resonance imaging to show that 12 weeks of olfactory training with those four scents could increase grey matter volume in olfaction-related brain regions (hippocampus and thalamus) in 30 patients with infection-related anosmia. A group of 31 similarly affected controls showed no brain changes on MRI (Gellrich J, et al. Laryngoscope. 2018).
Post-Viral Olfactory Dysfunction
SARS-CoV-2 is definitely not the only virus that can cause persistent post-viral olfactory dysfunction (PVOD), but it seems to be very, very good at it.
Partial or complete anosmia can occur following infections with rhinoviruses, parainfluenza virus, Epstein-Barr, and various other coronaviruses, including the 2002 SARS virus (Tian J et al. Laryngoscope. 2021). But anosmia is not nearly as common following any of these as it is following Covid.
The reasons for this difference are not fully clear. According to Dr. Koyama and colleagues, it may result from several factors: SARS-CoV-2’s propensity to replicate profusely in the upper airway before descending into the lungs; high expression of ACE2 receptors—the main viral binding site—on several types of olfactory epithelial cells (though not on olfactory neurons themselves); and the extremity of the immune system’s response to this particular virus, which can cause extensive damage to the olfactory epithelium.
A high number of the most severe Covid cases are in older people, and the epidemiological data suggest that long term olfactory damage is more common among elders. Epithelial repair capacity, which typically diminishes with increasing age, may be further impaired during the course of acute infection.
When assessing patients who have olfactory impairment seemingly related to Covid, it is important to rule out other potential causes. This usually requires nasal endoscopy to detect lesions in the nasal cavity or olfactory cleft; and a CT scan of the paranasal sinuses. Exposure to environmental toxins can sometimes cause anosmia, as can certain prescription drugs like nifedipine, phenothiazines, statins, and some antibiotics.
If there are no indicators of tumors or other physical obstructions, and no other obvious causes, then the next step is olfactory testing to measure olfactory thresholds and the ability to discriminate between different types of scents.
Olfactory Training After Covid
Late in 2020, Serge-Daniel Le Bon and colleagues at the Department of Otorhinolaryngology, Head and Neck Surgery, Université Libre de Bruxelles (ULB), Brussels, published a study of olfactory training with and without oral steroid therapy in a cohort of 72 Covid-19 patients.
More than one-third (27 of the 72) had persistent olfactory impairment following the acute Covid phase. Nine of them undertook smell training in conjunction with oral steroids, while 18 had the smell training alone.
For each therapy session, the patients sniffed the four key odors (rose, eucalyptus, lemon, cloves) for approximately 10 seconds each, twice daily, for 10 weeks. The oils were provided in a ‘Smell Training Kit’ made by Dos Medical-BV, Netherlands.
After 10 weeks, patients in the combination treatment group had significantly improved their olfactory scores by 7.7 points on average (p = 0.007), compared with a 2.1-point increase in those using smell training alone (Le Bon SD, et al. Eur Arch Otolaryngol. 2021).
The data “suggest the combination of a short course of oral corticosteroids and olfactory training is safe and may be beneficial in helping patients with enduring dysosmia recover from olfactory loss due to COVID-19.”
Unfortunately, there was no steroid-only group in this small pilot trial, so it is impossible to determine how smell training alone would compare to oral steroids alone.
Researchers at Benha University, Egypt, studied 50 post-Covid anosmia patients treated with smell training or a corticosteroid nasal spray (mometasone furate), 100 μg once daily for 3 weeks. They concluded that the steroid spray “offers no superiority benefits over the olfactory training, regarding smell scores, duration of anosmia, and recovery rates.” (Abdelalim AA, et al. Am J Otolaryngol. 2021).
Early on in the pandemic, the British Rhinological Society published consensus guidelines on Covid-associated smell loss that included a recommendation of olfactory training for “all patients with persistent loss of sense of smell of more than 2 weeks duration.”
That recommendation was based on the relative efficacy of smell training in other non-Covid types of PVOD, the wide prevalence of Covid-associated olfactory problems, and the recognition that there were no other effective treatments for this very common problem.
Massive Unmet Need
Olfaction is the least studied of the human senses. It was not until the mid 20th century that the basic mechanisms underlying the sense of smell were fully described. Even today, there are many unanswered questions.
Few physicians specialize in this field, and only a handful of major medical centers such as Stanford University and Vanderbilt University have dedicated clinics focused on olfactory problems. These clinics have been overwhelmed by post-Covid patients. Wait times for new appointments now exceed 6 months.
A recent article by CNN reporter Sandee LaMotte underscored the dire need for improvement of care for people with olfactory disorders.
Zara Patel, MD, a professor of otolaryngology at Stanford told CNN, “One of the big problems we realized at the beginning of the pandemic is that almost no one other than a few specialists knew anything about smell loss and how to go about diagnosing or treating it.”
Only a handful of major medical centers such as Stanford University and Vanderbilt University have dedicated clinics focused on olfactory problems. These clinics have been overwhelmed by post-Covid patients.

Patel is the lead author of a new international consensus statement on olfaction and olfactory disorders. This first-of-its-kind 600-page document drew input from 50 world experts, and attempts to make clinical sense out of the surge of olfaction research emerging from the Covid pandemic.
Patel and colleagues included olfactory training among their clinical recommendations for treatment of anosmia. Though the number of supportive studies is small, as are the cohort sizes, the available data make a reasonable case for use of smell training.
The guidelines note that the impact of smell training tends to be more definitive on subjective measures of olfaction, than on objective measures. That said, the authors point to studies showing structural changes in olfactory brain regions after prolonged training. This indicates that there can be objective anatomical and physiological changes.
Given the absence of other effective therapies, the negligible risk of worrisome adverse effects, and the low cost of olfactory training, the experts deem it worthy of consideration.
“We start with four odors that are in different categories of smell so that they will stimulate different types of olfactory receptor neurons in your nose: lemon, rose, eucalyptus and clove,” Dr. Patel told CNN. Patients should practice smell training twice daily for at least six months. It is definitely not a quick fix.
Neuroplasticity & Olfaction
Research on olfaction has grown exponentially in the wake of Covid. One of the most exciting lines of work is focused on neuroplasticity and olfactory function.
A team at Washington University, St. Louis, used resting state MRI to assess brain connectivity in 16 patients with anosmia, before and after 12 weeks of olfactory training. They compared the scans from the anosmic patients to similar MRI images from age and sex-matched control subjects with normal senses of smell. This led to some very interesting observations.
There were “significant differences in baseline brain connectivity between participants with PVOD and normosmic control participants…most notably with an increase in functional connectivity in the visual cortex” (Jiramongkolchai P, et al. JAMA Network. 2021).
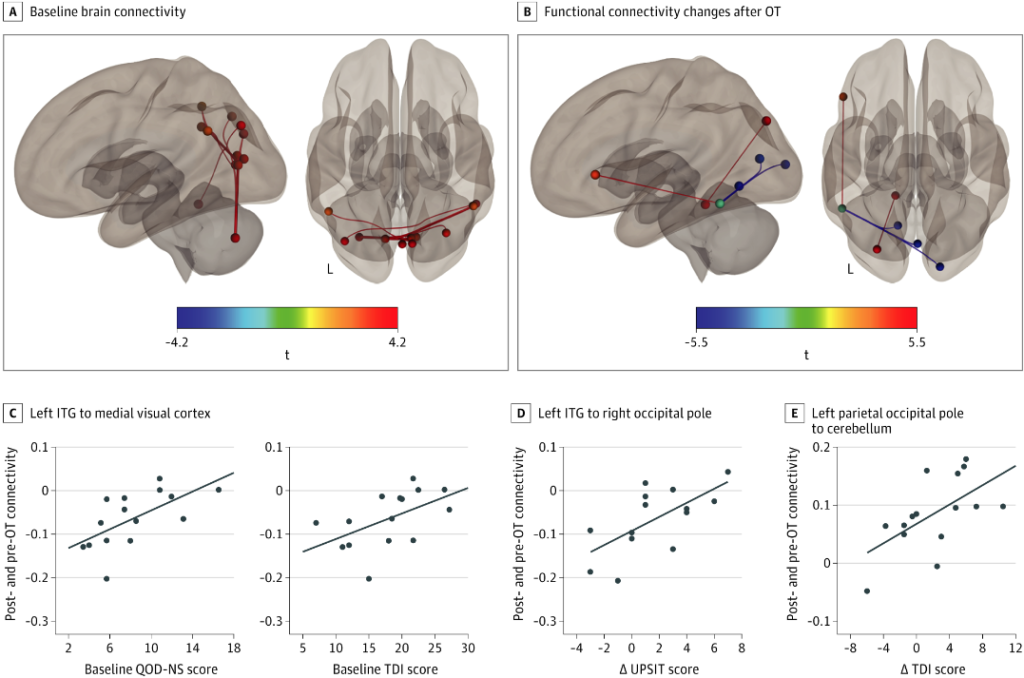
After 3 months of smell training, these brain changes normalized, as indicated by a decrease in the previously heightened visual cortex connectivity, and an increase in connections in the left parietal occipital junction and other brain regions involved in olfaction.
The findings imply that the olfactory and visual senses are closely connected, and olfactory training not only stimulates changes in olfactory function, it also impacts connectivity within the visual cortex.
After 3 months of smell training, brain changes normalized, as indicated by a decrease in the previously heightened visual cortex connectivity, and an increase in connections in the left parietal occipital junction and other brain regions involved in olfaction.
“Loss of a vital organ sense may lead to adaptation, remodeling, and heightening of a closely related sense, namely, vision,” the authors wrote. “This case-control cohort study suggests that there is a visual connection to smell that has not been previously explored with olfactory training and that further studies examining the efficacy of a bimodal visual and olfactory program are needed.”
Future Directions
According to Dr. Koyama, and her colleagues in the US and Japan, olfactory training is ripe for expansion beyond the simple four-constituent model that has been in use since Henning’s day.
Every aromatic plant contains hundreds if not thousands of flavonoids, terpenes, and other potentially bioactive compounds. The characteristic scent of a plant is determined by multiple constituents, not single compounds.
In a recent paper, Koyama and co-author Thomas Heinbockel suggest that olfactory training exerts its effects through multiple biochemical mechanisms.
“Possibly, the essential oils contain chemical constituents with bioactive properties that facilitate the recovery of the olfactory sense by suppressing inflammation and enhancing regeneration.” (Koyama S, Heinbockel T. Front Pharmacol. 2022).
Some essential oils may have intrinsic antiviral and anti-inflammatory properties. Others are analgesic or anxiolytic, which could be a big plus given that anosmia can cause significant distress.
Koyama and Heinbockel identify 11 common essential oils– mulberry, licorice, turmeric, lavender, thyme, summer savory, lemongrass, tea tree, oregano, mint, and peppermint—that contain at least five anti-inflammatory compounds, and one or more that are directly anti-viral. Others, such as hinoki cypress, summer savory, and cinnamon have high numbers of anti-viral compounds.
“It is important to understand and consider the bioactive properties of the chemical constituents of the essential oils when they are used in smell training. Many terpenes activate multiple pathways. It is important to know the major chemical constituents in the essential oils and to understand their effects as well as the pathways that they activate in order to utilize the essential oils in the most effective way.”
By identifying the myriad compounds in these plants and the human biochemical and neurological pathways they activate, researchers can lay groundwork for what Koyama calls “precision olfactory and taste training”—the targeted and individualized use of specific plant scents to elicit specific therapeutic responses.
END


