The Long Covid nutritional protocol developed by the 10-member practitioner working group under the aegis of OvationLab and ANDHealth, is divided into two parts—Foundational Supplements aimed at improving overall health, and Specialty Supplements focused on the five main drivers of Long Covid: ACE2-mediated tissue damage; viral persistence; chronic inflammation; mitochondrial dysfunction; and microbiome/dysbiosis.
The working group is continually re-evaluating and refining the protocol and dosing schedule.
The
Foundational Supplement protocol includes:
MitoCore (Ortho Molecular Products): a comprehensive multivitamin that also contains N-acetyl cysteine (NAC), Glucoraphanin, Alpha lipoic acid (ALA), Resveratrol, Epigallocatechin gallate (EGCG), Acetyl L-carnitine, Manganese, and Zinc. The working group recommends 2 caps, twice daily for 90 days.
OmegaGenics (Metagenics), a concentrated Omega-3 product containing 710 mg EPA and 290 mg DHA; 1,000 mg twice daily for 90 days.
Magnesium Glycinate, 200 mg twice daily for 90 days
Co-Enzyme Q10, 200 mg per day, for 90 days
Quercetin, 500 mg, twice daily for 90 days
Vitamin K2 with D3: Up to 10,000 IU daily, with specific dosing based on each patient’s serum levels. If the serum level is below 40 ng/ml, use 10,000 IU. If it’s within 40-60 ng/ml, use 5,000IU. If above 60 ng/ml, the patient does not need supplementation.
The
Specialty Supplement protocol consists of:
Arterosil (Calroy Health Sciences): The main
constituent in Arterosil is Rhamnan sulfate,
a
sulfated polysaccharide from two types of marine algae (Monostroma
Latissium and Monostroma Nitidum). Rhamnan sulfate has a similar
structure to glycosaminoglycans found in the human endothelial glycocalyx—the thin
gel-like layer that coats the luminal surfaces of healthy blood vessels. Glycocalyx
damage is
one of the earliest steps in the pathogenesis of cardiovascular disease, and it
is a
common consequence of Covid.
“In
order to have any hope of repairing tissue damage, we need optimized blood flow
and optimized vessel health. Arterosil targets the regeneration and repair of
the endothelial glycocalyx,” said Kristine Burke, MD, a co-chair of the PVRP
Working Group, during a
webinar outlining the protocols.
ITIS (Return
Healthy): This product is a
complex of anti-inflammatory herbs, including Skullcap (Scutellaria
baicalensis), Curcumin (Curcuma longa), Frankincense (Boswellia
serrata) and others. Dr. Burke noted that Scutellaria produces a compound
called Baikalin that is able to cross the blood-brain barrier, making the
product useful for mitigating the cognitive impairment, mood disturbances, and
“brain fog” that many Long Covid patients experience. That’s in addition to the
product’s capacity to reduce systemic inflammation, one of the main drivers of
the post-viral syndrome.
Tollovid (Todos Medical): This unique substance is derived from an herb
called Lithospermum erthythrorhizon, known colloquially in English as
Gromwell root, or Zicao in Traditional Chinese Medicine.
“Tollovid
addresses persistent viral infections by blocking viral replication capacity,”
explained Dr. Burke.
It does this by binding tightly to the 3CL protease, an enzyme that coronaviruses use to cleave the long polypeptide chains produced from their mRNA during the replication process. Tollovid is among a number of 3CL inhibitors being explored in the Covid context. Essentially, it shuts down the replication process.
MegaSporeBiotic (Microbiome Labs): This probiotic
product delivers spores from five strains of Bacillus subtilis. PVRP
Working Group members believe it is ideally suited to address the marked
microbiome alterations associated with Covid and sometimes, Covid vaccination.
“We want to recondition the gut and bring back a healthier microbiome,
especially facilitating the resurgence of those species that are important in
immune regulation,” Burke said.
Rather than “seeding” the gut with exogenous probiotic organisms, the goal of treatment with a spore-based product like this is to shift the microbial ecology so that it favors growth and flourishing of a patient’s own endogenous bacterial species.
MegaPre (Microbiome Labs): A prebiotic product containing three different types of non-digestible oligosaccharides derived from kiwi fruit, nonGMO corn cobs, and rBST-free cow’s milk. Supplementation with this combination increases GI microbial diversity and selectively feeds beneficial organisms like Akkermansia muciniphilia, Faecalibacterium prauznitzii, and various species of Bifidbacteria which, Dr. Burke noted, are often decimated by SARS-CoV-2 infection.
“We found ourselves needing a curated suite of nutritional product solutions that were targeted at the five main drivers of Long Covid: ACE2 mediated damage/tissue damage; viral persistence; chronic inflammation; mitochondrial dysfunction; and microbiome/dysbiosis.”
–Kristine Burke, MD
For
the first 30 days, in addition to the full array of Foundational supplements,
patients should take: Arterosil, 2 caps twice daily; ITIS, 2 caps thrice daily;
Tollovid 3 caps 4 times per day; and MegaSpore alone (the prebiotic is added
later), 1 cap daily for the first 7 days, and then 2 caps daily until the
bottle is finished.
From Day 30 to Day 90, patients can cut the doses to: Arterosil 1 cap twice daily; and Tollovid 1 cap twice daily for 30 days. They should eliminate the MegaSpore probiotic, replacing it with the MegaPre oligosaccharide formula, 3 caps per day.
All products in the protocols are available as a bundle from Fullscript. Practitioners with Fullscript accounts can prescribe the complete protocols for patients, and Fullscript will deliver the full product suite to their homes, along with detailed implementation instructions.
Dr.
Burke and members of the Working Group stress that the current protocols,
though based on a scientific review of hundreds of potential candidate products,
are still a work in progress. The team has established a standardized registry
to track outcomes in hundreds of patients now on the protocols, and they will
use the data to revise the protocols if necessary.
She
added that these regimens are flexible. “There may be some patients for whom we
want to add some other tools not on the protocol list. You may choose to add or
subtract products. But this is the broadest and simplest set of products and
processes that we could develop. We’re not promoting specific brands
necessarily. But the ones on the list, we found data to support the use of each
of them to target one or more of the five key drivers of long Covid.”
Disclosure: ANDHealth and Calroy Health Sciences are clients of OvationLab.
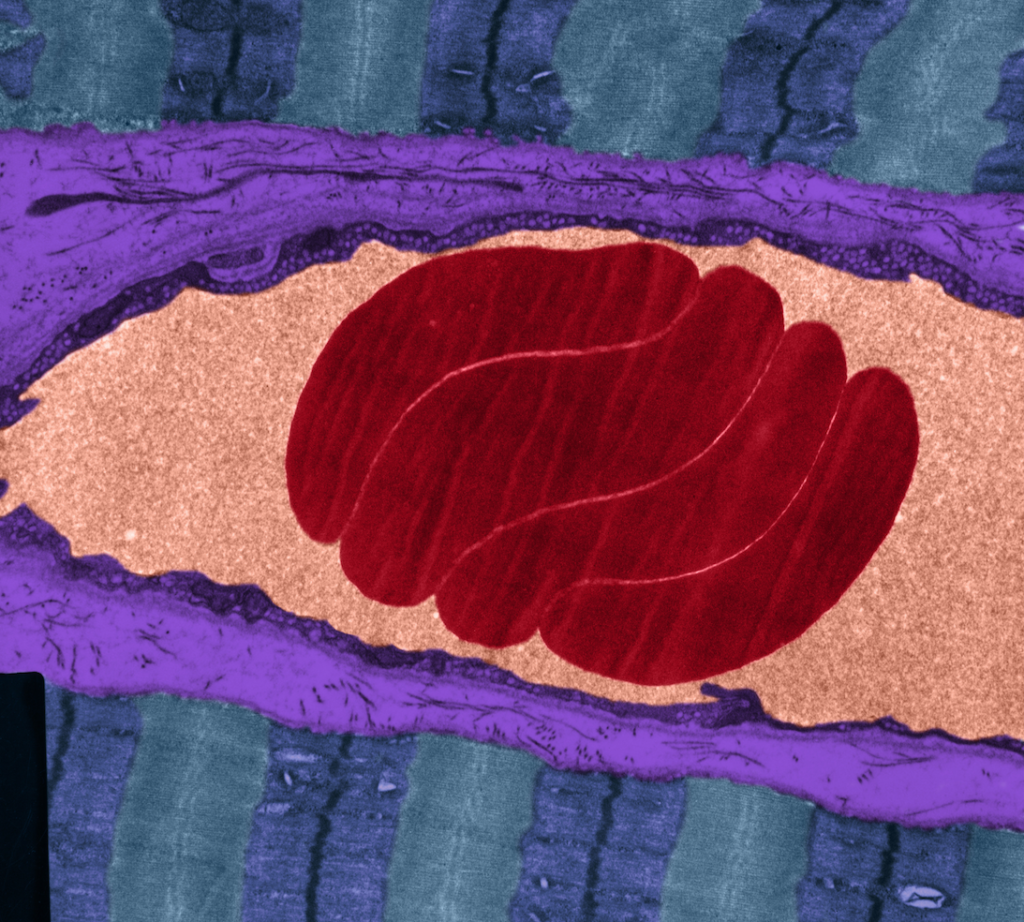
Transmission electron micrograph of capillary, with four erythrocytes. The outer surface of the endothelial cells is coated by an electron-opaque glycocalyx (purple). Glycocalyx damage is the earliest step in the progression to atherosclerosis. (Image: OMIKRON/Science Photo Library)
Repair
of the endothelial glycocalyx is a vital element in the restoration of
cardiovascular health, according to Mark Houston, MD, director of the
Hypertension Institute at Saint Thomas West Hospital, Nashville.
The endothelial glycocalyx (EGX) —literally “sugar coating” in
Greek—is a very thin gel-like layer that lines the luminal surface of the blood
vessels. It is a carbohydrate-rich mesh of membrane-bound and soluble
glycoproteins, proteoglycans, and glycosaminoglycans, which create a
non-adherent shield.
Damage to this sensitive, bioactive layer is one of the earliest
steps in the pathogenesis of cardiovascular disease, Dr. Houston said at the
2022 Integrative Healthcare Symposium.
“Endothelial
dysfunction is the starting point of CVD, and the EGX is the primary protector
of the endothelium. Therefore, maintaining a healthy EGX may be one of the most
important intervention targets for prevention of CVD.”
A “SMART”
Barrier
To
understand the importance of the EGX keep in mind that the vascular endothelium
is not passive. It actively controls passage of nutrients, oxygen, and hormones
into and out of the bloodstream. It is also a key player in immunity and
inflammation. Through production of nitric oxide, it regulates blood pressure.
“The
endothelium affects the structure and function of every other organ system,”
Houston explained. “Whatever the glycocalyx does, the endothelium does as
well.”
According to Dr. Houston, the glycocalyx is a “SMART” barrier:
Selective: It is selectively
permeable, preventing cholesterol, platelets, leukocytes, and other circulating
blood components from sticking to vessel walls, but allowing passage of
nutrients, dissolved gases, and signaling molecules.
Micro-thin: The thickness of the EGX
varies with the thickness of the arteries it coats. It is generally in the
range of 2-3 um in small vessels, and up to 4.5 um in larger ones like the
carotids. Even at its thickest, it is still quite thin. It would
take roughly 1,000 layers of EGX to equal the thickness of one sheet of paper.
Antioxidant:
The
EGX harbors the
antioxidative enzyme, superoxide dismutase (SOD), which reduces oxidative
stress, and keeps nitric oxide (NO) available to the vasculature.
Regulator: It regulates vascular
permeability, inflammation, coagulation, and fluid balance.
Transducer: The
EGX contains
brush-like structures in the 150-400 nm range, comprised of glycoprotein and
proteoglycan chains. These sense the shear stress of blood flow, and signal
the endothelium to produce nitric oxide when needed to regulate vascular tone.
It also responds to chemokines, cytokines, and other molecular signals involved
in vascular homeostasis.
Mark Houston, MD
One
of its primary functions is to protect the endothelium from thrombus formation.
It blocks the binding of sticky leukocytes, activated platelets, and
lipoproteins–especially LDL. It also contains anti-thrombin III, tissue factor
pathway inhibitors, lipoprotein lipase, vascular endothelial growth factor,
superoxide dismutase, and hyaluronic acid, all of which mitigate inflammation
and resist thrombus formation.
Negatively
charged glycosaminoglycans within the EGX bind and inactivate sodium, rendering
it non-osmotic and preventing it from accumulating in the endothelium. Thus,
the EGX buffers against salt-induced arterial stiffness.
Hyperglycemia
& EGX Damage
Damage
to the EGX is a direct consequence of persistent hyperglycemia, dyslipidemia,
chronic inflammation, and oxidative stress. It precedes all the vascular
complications of diabetes.
“Endothelial dysfunction is the starting point of CVD, and the EGX is the primary protector of the endothelium. Therefore, maintaining a healthy EGX may be one of the most important intervention targets for prevention of CVD.”
Mark Houston, MD, Director, Hypertension Institute at Saint Thomas West Hospital, Nashville
“High
blood glucose causes damage to glycocalyx, even in the so-called “normal”
range. You want fasting blood sugars down to 75, and the A1c down to 5. Anything
above that will increase risk because that’s when the glycocalyx damage starts,”
Houston told IHS attendees.
Many
other things also contribute to glycocalyx degradation, including elevated TNF-a,
hypervolemia, low fluid sheer stress, elevated hyaluronidase, matrix
metalloproteinases, atrial natriuretic peptide, and bacterial endotoxins.
There’s
a clear and simple correlation between reduced EGX thickness and predisposition
to lesion formation. Houston noted that in “atheroprone” regions of the
vasculature–such as vessel branches, bifurcations, and curvatures—the EGX is
typically very thin.
Restoring
the Glycocalyx
A number of treatments and factors can help to restore, regenerate,
or maintain a healthy EGX, including:
Hydrocortisone
Calcium channel blockers
Glycemic control via Metformin
Sulodexide—a highly purified mixture of glycosaminoglycans
composed of low molecular weight heparin (80%) and dermatan sulfate (20%)
Statins
Reduction of inflammatory mediators
Nitric oxide
Albumin
Fresh frozen plasma (FFP)
N-acetyl cysteine (NAC)
Hydroxyethyl starch
Sphingosine-1
phosphate (SIP)
Glycocalyx-regenerating compounds (GRCs): hyaluronan,
antithrombin III, heparin, sulodexide, specialized sulfated polysaccharides
(SSP), and protein C
But Dr.
Houston holds that the single most effective and convenient option is Rhamnan
sulfate (RS),
a sulfated polysaccharide
extracted from two types of marine algae (Monostroma Latissium and Monostroma
Nitidum). These polysaccharides
have similar structure to
glycosaminoglycans found in the human EGX.
Rhamnan Sulfate: Safe & Effective
Early
in vitro experiments showed clearly that rhamnan sulfate can repair EGX
damage caused by excessive glucose exposure. Animal experiments show that it
prevents leukocyte adhesion, suggesting that it might prevent endothelial
inflammation at its earliest stages.
Rhamnan
sulfate is available as a dietary supplement called Arterosil. This product also contains
grape seed extract, green tea extract, and concentrated extracts
from a host of heart-healthy fruits and vegetables.
Supplementation
with rhamnan sulfate can markedly increase arterial elasticity, a good
indicator of endothelial function. In a study of 19 healthy humans at Baylor College
of Medicine, daily supplementation with Arterosil increased carotid arterial
elasticity by an average of 89.6% over baseline, within two hours of ingestion.
“Arteries
are arteries. If it does this in the carotids, my guess is that it does it
everywhere,” said Dr. Houston. “If you give a glycocalyx promotor, you can get
increases of vascular compliance very quickly, and the functional changes beget
structural changes.” He added that he is now recommending Arterosil and other
glycocalyx-promoting treatments to 100% of the patients in his clinic.
“The
average increase in arterial elasticity is almost 90%, very significant improvements.”
Plaque
Reversal
Houston
contends that conventional medicine’s myopic obsession with lipids has blinded
many physicians to the myriad other factors that drive vascular pathology.
“Even
if you use statins and drive down LDL to 40, still 50% of patients will have
events. Lipids are not the only problem in CAD. There are many other steps.”
That
said, new evidence
indicates
that rhamnan sulfate can reduce atherosclerotic plaque formation, at least in
mice. Notably, the plaque-reducing and
anti-inflammatory effects were stronger in female versus male animals.
Dr.
Houston reported early data from an ongoing human pilot study of rhamnan
sulfate in patients with vulnerable atherosclerotic plaques, as confirmed by MRI-PlaqueView imaging. PlaqueView
is the only FDA-approved software system for carotid plaque analysis.
He
pointed out that stenotic plaques account for less than 50% of all “culprit”
lesions, whereas 75% of all events are attributable to ruptured non-stenotic
plaques that trigger thrombus formation.
Daily
supplementation with a rhamnan sulfate product for two months led to a mean 64%
regression of lipid-rich necrotic plaque—the most dangerous type of plaque—in
the female participants, and a 47% regression in the males. There were also significant increases in
vessel lumen diameter, suggesting a reduction of carotid stenosis—a finding
that has not been observed in statin studies.
“Rhamnan
sulfate changes the morphology of plaques, making them more stable. These are
very significant changes. Nothing else does this. No drug can do this. Statins
reduce lipid-rich necrotic plaques by about 25%, which is meaningful, but not
even close to what you get with the Rhamnan sulfate.”
These
preliminary findings from China, have prompted a larger US-based study which is
now underway.
Houston
stressed that plaque reversal is a gradual process. Typically, it takes about 6
months of twice-daily dosing to see reversal of carotid plaques. “For really
bad cases, you can take two caps, twice daily. The key is to split the doses,
ideally 12 hours apart. It works better that way.”
“Rhamnan sulfate changes the morphology of plaques, making them more stable. These are very significant changes. Nothing else does this. No drug can do this. Statins reduce lipid-rich necrotic plaques by about 25%, which is meaningful, but not even close to what you get with the Rhamnan sulfate.”
Mark Houston, MD, Director, Hypertension Institute at Saint Thomas West Hospital, Nashville
Rhamnan
sulfate does not break up plaques and cause fragments to float away. Rather it
promotes resorption of the lipid core while simultaneously blocking deposition
of lipids. It does this without actually affecting serum lipid levels.
According
to Dr. Houston, Aterosil is safe, and unlikely to interact adversely with
medications. In fact, it is likely to be synergistic with Rosuvastatin
(Crestor) and other statins. “There are zero drug interactions with this. In
combination with nearly everything we use, the interactions are generally good.
If anything, it makes the drugs more effective.”
Impact
on Blood Pressure
Houston and his colleagues at the St. Thomas West Hospital studied Arterosil in a cohort of ten patients with uncontrolled hypertension. After three months of twice-daily dosing, the patients showed a decrease in mean systolic pressure from 151.5 mmHg at baseline, down to 147.5 at the three-month point. Diastolic pressure dropped from a baseline mean of 93.2 down to 82.3 mmHg.
His
team is currently looking at the impact of this product on diabetic neuropathy
in a cohort of 20 patients. He says “preliminary results are very promising.”
Potential
Role in Covid Care
The glycocalyx
and its restoration has implications in the context of Covid-19.
A
healthy EGX may reduce susceptibility to viral infection, as well as the risk
of severe Covid symptoms if one does get infected. Conversely, the Covid
disease process can damage the glycocalyx, Dr. Houston explained.
Early
on in the pandemic, investigators at the Lawson Health Research Institute,
Ontario, reported that ICU patients infected with the then-novel virus showed
marked glycocalyx degradation compared with ICU patients who were virus-negative.
This correlated with increases in thrombosis, depressed nitric oxide
production, and increased platelet adhesion (Fraser
DD, et al. Crit Care Explor. 2020).
“A therapeutic strategy based on glycocalyx protection would be effective for Covid-19 patients with both early and severe (e.g., ARDS) disease.”
Hideshi Okada, MD, Gifu University, Japan
A
team at the Jagiellonian University, Krakow, Poland showed that in human
pulmonary arteries, the intact EGX strongly binds viral spike protein, “but
screens its interaction with ACE2.” When the glycocalyx is reduced, ACE2
receptors on the surface of the endothelial cells are exposed, enabling the
spike proteins to bind. The Krakow group concluded that susceptibility to Covid-19
may depend on the condition of the glycocalyx.
A Greek
research team showed strong correlations between reduced EGX thickness,
oxidative stress, vascular dysfunction, and impaired cardiac performance in
patients with SARS-CoV-2.
Dr.
Houston noted that “even in mild cases of COVID-19, EGX damage can persist for
up to four months, and has been correlated with a 10-fold elevation in
oxidative stress compared to controls. If the ACE2 enzyme is low to begin with, something like Covid,
which depletes ACE2, will cause big, big problems. This is what happens in very
bad cases.”
It
is notable that people on ACE2-sparing drugs tend to have milder Covid cases. “You
can increase the effects of ACE2 with a glycocalyx promoter,” Houston says.
In
their excellent review of vascular injury in Covid-19, Dr. Hideshi Okada and
colleagues at the Gifu University, Japan, point out that the endothelial
glycocalyx is already very thin in pulmonary capillaries. Further degradation
following an inflammatory cascade could be a major factor in acute and
long-term Covid (Okada H, et al.
Microcirculation. 2020).
“A therapeutic strategy based on glycocalyx protection would be effective for Covid-19 patients with both early and severe (e.g., ARDS) disease,” writes Okada. “A patient with comorbidity such as diabetes or hypertension would most likely exhibit an impaired glycocalyx function. Accordingly, their endothelial cells would not be fully protected and would be more susceptible to external (or internal) pathogens. In other words, the prevention of endothelial glycocalyx injury represents a useful means of systemic defense against infection.”
Blocking Viral Entry
Researchers at the Rensselaer Polytechnic Institute showed in
cell culture experiments that rhamnan sulfate binds the spike protein binding
domains on SARS-CoV-2, inhibiting interaction with ACE2 and heparan sulfate on
endothelial cell surfaces. The effect of the seaweed extract was stronger than
that of heparin or of pseudoviral particles being tested as potential Covid
treatments.
The Rensselaer team reported strong antiviral activities against
wild type SARS-CoV-2 as well as the delta variant (Song Y, et al. Mar
Drugs. 2021).
Animal
experiments at Chubu University in Japan suggest that rhamnan sulfate can
directly inhibit influenza virus infection, while also promoting antibody
production (Terasawa
M, et al. Mar Drugs. 2020). They conclude that it is a potential
candidate for the treatment of influenza virus infections