The COVID pandemic has clearly underscored the consequences of
another American health crisis: the obesity epidemic. And it further emphasizes
the necessity for integrating sustainable lifestyle practices that promote
general health and wellbeing.
In a sense, COVID tells a tale of two pandemics: one infectious,
and one chronic and longstanding.
The SARS-CoV-2 virus has permeated our everyday life for two years
now, and many of our patients have had drastic changes in their lifestyles as a
result. Community activities shut down, gyms closed, and many people became
more sedentary. A lot of people started working from home, thus reducing their
already minimal daily walking and movement. Even shopping has shifted online,
and many people need only walk from the couch to the front door or the curbside
to pick up their deliveries.
Putting it simply, the pandemic has rendered many of us inactive, which
is furthering our already alarming obesity rate. And we know that obesity and
its related metabolic disorders are major COVID risk factors.
The CDC reports that in 16 of the 50 states, 35% or more of
all residents are now obese. That’s up from 2018, when 9 states had a 35%
prevalence. A CDC-sponsored study of more than 540,000 hospitalized patients
hospitalized showed that COVID-19 was linked to underlying conditions such as
obesity, diabetes with complications, and anxiety disorders were the strongest
risk factors for severe COVID and death.
What we have here is a vicious cycle: Obesity predisposes people to
a severe COVID, but strategies aimed at preventing transmission of infection
(work from home, online shopping, shuttering of social and recreational
activities) promotes obesity.
To help our patients navigate this tumultuous time, we need to address
both of these pandemics, and teach people about lifestyle factors that can
reduce the risk of both.
Here are five sustainable ways for your patients to transform their
health, maintain a healthy weight, and support their immune system.
High-Protein Breakfast: Patients often come to us for
dietary guidance. One of the best pieces of advice we can share is to eat a
higher protein breakfast.
A 2015 study of 28 overweight but otherwise healthy adolescents
showed that eating a daily breakfast containing at least 35 grams of protein,
can reduce 24 hour glucose variability, daily glucose peaks, and post-prandial
glucose fluctuations (Bauer
LB, et al. Int J Obes. 2015). It improves overall glucose
control, thereby helping people maintain or work toward health weight.
Of course it is also important to minimize fast foods, processed
foods, and products laden with added sugars, artificial sweeteners, and trans
fats.
Physical Activity: Working out is an excellent way to
lower obesity in the population. I believe it is part of our job as physicians
to make sure that our patients engage in a workout routine of some sort that
they enjoy and that won’t lead to fatigue or injury.
The American Heart Association recommends that healthy adults get
150 minutes (30 minutes, five days a week) of aerobic activity. This is easily
accomplished with a 30-minute walk after dinner. If someone can’t walk for 30
minutes straight, break it out into three 10-minute walks, or two 15-minute
walks.
If a patient has been completely sedentary, it’s best to ease into
physical activity rather than immediately jumping into an intensive routine.
The main thing is to get people moving. Moderate exercise is crucial during
this prolonged pandemic.
A recent Kaiser Permanente analysis of data from more than 48,000
COVID patients showed that those who were routinely inactive had significantly
higher risk for severe Covid-19 outcomes (hospitalization, ICU admission,
death) than those who consistently met basic physical activity guidelines (Sallis R, et al. Br J
Sports Med. 2021).
Optimize Sleep: The CDC recommends that adults aged 18-60 years get seven or more hours of
sleep per night. The reality is that our patients might be sacrificing sleep to
accomplish other goals such as work, social or familial responsibilities.
Sleep is essential for physiological and neurological rest and
repair. It also plays a central role in maintaining healthy weight and sleep
deprivation impedes the ability to lose weight.
University of Chicago researchers showed that people sleeping 8.5
hours lost 55% more body fat than those sleeping an average of 5.5 hours, while
following exact same moderately restrictive diet (Nedeltcheva AV, et
al. Ann Intern Med. 2010).
More than 20 chemicals have been identified as obesogens, many of
which are estrogenic in that they easily bind to estrogen receptors. The five obesogens most commonly found in
the home are Bisphenol-A (BPA), Phthalates, Atrazine, Organotins, and
Perfluorooctanoic Acid (PFOA).
Reducing exposure to these chemicals is as simple –or as complex—as
paying attention to the types of personal care, cosmetics, and household
products one purchases. Choosing the ones that are free from some or all of
these compounds. It is also wise to minimize the use of plastic containers for
food storage or preparation, since plastics are a major source of obesogenic
substances. Glass, stainless steel, and ceramic options abound, and they are
much safer.
Optimize Vitamin D Levels: For overall
health improvement, this is one of the easiest changes to implement. Taking a
vitamin D supplement is a completely sustainable habit that can have a
tremendous impact on patient health, especially for people living in northern
latitudes that do not get as much sun exposure.
There’s ample evidence that low vitamin D correlates with high
COVID risk. A study from the first year of the pandemic showed that vitamin D
deficiency was associated with a six-fold increase in severe disease from COVID-19
and 15-fold risk of death, so this is a healthful, timely and easy resolution (Radujkovic A, et al. Nutrients.
2020). Since then, many other studies have been published, from all over
the world, showing this inverse correlation.
Beyond vitamin D, many other nutrients can be helpful for immune
system support. Getting a better snapshot of your patient’s immune system can
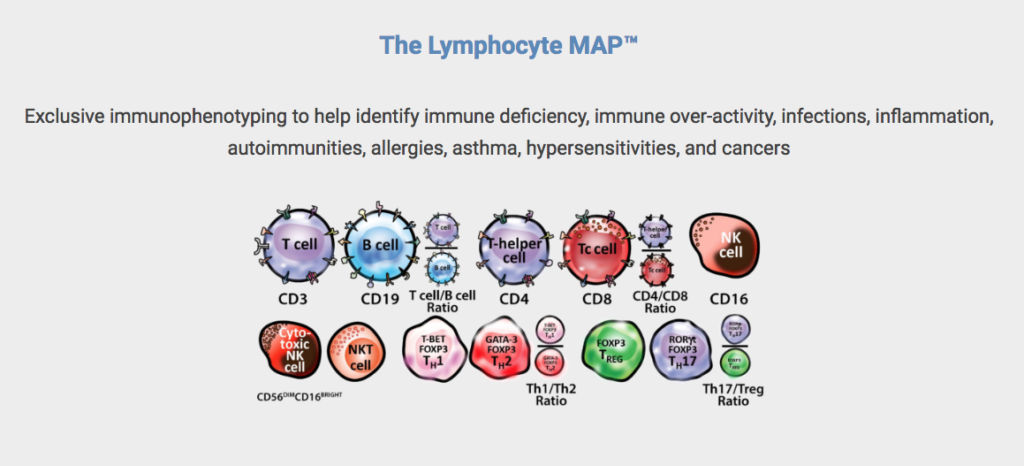
help you to tailor your suggestions. Cyrex Laboratories, a clinical laboratory specializing
in functional immunology and autoimmunity, has developed a test panel called
the The Lymphocyte MAP™.
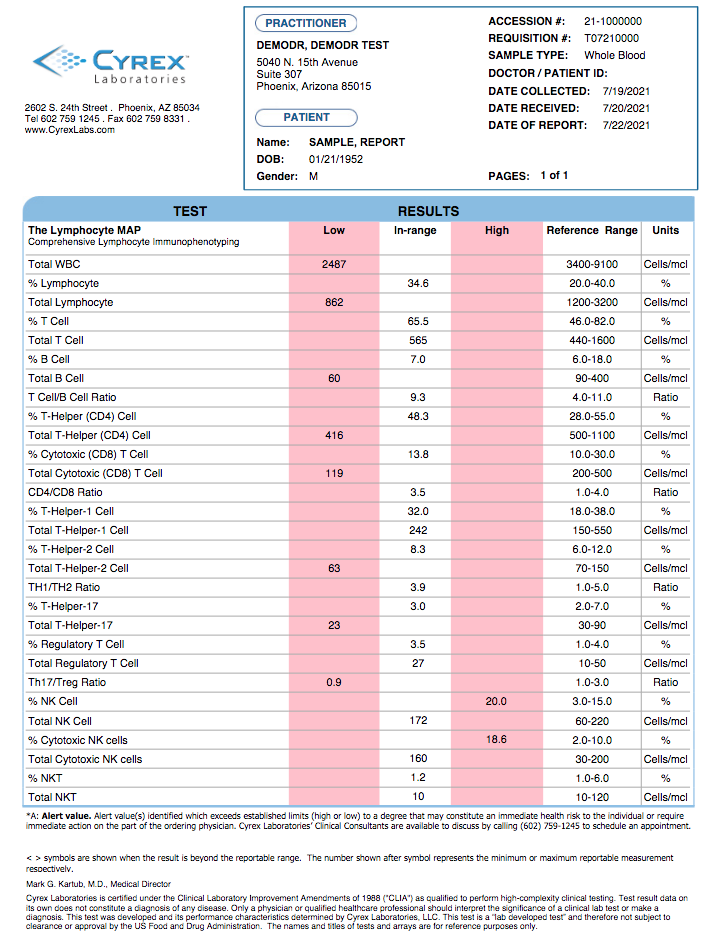
The Lymphocyte MAP screens the integrity of the immune system to define
a patient’s immune status and immunotype(s) based on 29 key biomarkers and
determinants. It tells you a lot about the current status of a patient’s immune
system so that you can provide guidance on adjustments that will bolster immune
response.
As the COVID-19 pandemic continues to surge, this can be vital
information as we work to help our patients fight not only the virus, but the
broader pandemic of obesity and metabolic dysregulation.
END
Dr.
Chad Larson, NMD, DC, CCN, CSCS, Advisor and Consultant on Clinical Consulting
Team for Cyrex Laboratories. Dr. Larson holds a Doctor of Naturopathic Medicine degree from
Southwest College of Naturopathic Medicine and a Doctor of Chiropractic degree
from Southern California University of Health Sciences. He is a Certified
Clinical Nutritionist and a Certified Strength and Conditioning Specialist. He
particularly pursues advanced developments in the fields of endocrinology,
orthopedics, sports medicine, and environmentally-induced chronic disease.
As we head into the peak months for the flu, we as health care providers need to
be especially vigilant about the integrity of our patients’ immune systems.
Paired with COVID-19, this year’s flu season carries the serious risk of
compromising their future immune response.
A key step in preventing these complications lies in
helping our patients understand the strengths and weaknesses of their immune
systems. Being more aware of their individual vulnerabilities will equip them
with an additional line of defense during the dangerous winter months.
With advanced
tools like immunophenotyping, we will be better able to advise patients about
ways to protect themselves against the threat of serious illness.
Because widespread social distancing and mask measures brought about an historic decrease in influenza transmission last year, population immunity is also likely to be lower than it has been.
A Brutal Flu Season
This
year’s flu season is anticipated to be particularly severe, and with COVID-19
still spreading in communities across the country, the stage is set for an
impending “twindemic.”
Because
widespread social distancing and mask measures brought about an historic decrease in influenza transmission last year, population immunity is also
likely to be lower than it has been, according to the Centers for Disease Control and Prevention (CDC) and National
Foundation for Infectious Diseases (NFID). As such, everyone is at increased
risk of contracting the flu during the 2021-22 season.
Even in
milder years, the flu has a significant impact on hospitalization and mortality
rates. According to the CDC’s estimates based on preliminary data from the 2019-20 season ending just prior to broad adoption of COVID-19 precautions,
there were approximately 35 million people with symptomatic illness, 380,000
hospitalizations and 20,000 flu-related deaths in the US.
With the
flu and COVID-19 both circulating and potentially peaking simultaneously in
early winter, a large population of the country is under high risk
of co-infection. This can not only aggravate
the
symptoms and complications of disease, but also create treatment conflicts for
individuals who are hospitalized.
For
example, corticosteroids, administered to prevent or mitigate severe COVID-19-related inflammatory
responses, are associated with poor outcomes and increased mortality in severe
influenza patients.
Assessing
the Immune System
With both
viruses triggering immune responses that affect vital organs, including the
lungs, brain, heart, and muscle, we are concerned about the long-term risks
that co-infection brings to the immune system.
We know that people with weakened immune systems due to
preexisting disease or exposure to certain medications are at a higher risk for
complications from both the flu and COVID-19.
Recent research has also shown the ability of SARS-CoV-2 to
hyperstimulate the immune system and trigger flares of pre-existing autoimmune reactions, even among those who
previously showed no overt symptoms of autoimmune disease. Many of our patients
could unknowingly be immunocompromised and at risk of severe illness in the
event of co-infection this flu season.
With the flu and COVID-19 both circulating and potentially peaking simultaneously in early winter, a large population of the country is under high risk of co-infection.
A complete blood count (CBC) done as part of routine blood work, is
frequently the initial diagnostic tool for identifying immunological disorders.
But it is only a
small part of a complex map that helps our patients understand their immune
systems and potential weaknesses.
CBCs alone are insufficient and incomplete for helping us
determine how vulnerable our patients are to opportunistic viruses. Looking
at a patient with an inflammatory disorder, for example, white blood cell (WBC)
and total lymphocyte counts could both come back as “normal” on a routine CBC, indicating nothing out of the ordinary, despite
the fact that the patient is actually suffering from dysregulation of the
immune system.
In fact, most immunologists agree that even in patients who have been
diagnosed with immune-mediated conditions like allergies, rheumatoid arthritis,
and neuropathies, the CBC is normal about 70 percent of the time.
Immunophenotyping
for Flu Protection
Being able to detect early immunological warning
signs and risk goes a long way in helping patients understand the functions and responses of their immune systems. We
can offer this support by looking at immunophenotype patterns, or immune system
“fingerprints,” which paint a much clearer picture of immunological makeup.
Immunophenotyping provides critical
information about immune cells and how well they work together. The techniques
are based largely on flow cytometry, which isolates and quantifies different
types of cells based on antigens and markers present on the cell surface.
Advanced flow cytometry can precisely measure the properties of living cells
such as size, shape, density, and granularity, with a high degree of precision.
Lymphocytes represent 20% to 40% of a patient’s total WBCs. By quantifying these subpopulations and the ratios between them, we are better able to predict how an individual might react to environmental antigens like influenza viruses.
Immunophenotyping by flow cytometry is useful
in the identification and quantification of lymphocyte subsets. This is
especially valuable when working with patients whose CBCs are normal.
Immunologists have found that about half of those with normal CBC values will show
immune abnormalities when flow cytometry is used to quantify T-cell, B-cell, NK
cell, CD4, and CD8 lymphocyte populations.
Flow cytometry is widely used in cancer
research. The accuracy and detail provided by these tests have demonstrated
significant value well beyond oncology.
Lymphocytes represent 20% to 40% of a
patient’s total WBCs. By quantifying these subpopulations and the ratios
between them, we are better able to predict how an individual might react to
environmental antigens like influenza viruses.
Comprehensive
Immunophenotyping
Knowledge gained through
immunophenotype patterns is essential for physicians wishing to offer better
immune system support, including helping immunocompromised patients make
informed decisions during critical periods like flu season.
Cyrex Laboratories, a clinical laboratory specializing in
functional immunology and autoimmunity, has recently developed a proprietary
test panel called The Lymphocyte Map – Comprehensive Immunophenotyping of
Lymphocytes. This tool provides a much more comprehensive
evaluation of the immune system than a CBC, providing greater clinical insight
about a patient’s immune susceptibility.
By measuring the integrity of the immune
system at the cellular level, based on 29 key biomarkers, The Lymphocyte Map allows providers to classify a patient’s
immunophenotype patterns into 13 different immunotypes. This can reveal hidden
patterns and trends regarding immune system weaknesses, imbalances, and overall fitness.
Practitioners can also use
immunophenotypes to design treatment plans to reduce or prevent the progression
of disorders and mitigate the influence of exogenous pathogens.
Now, more than ever, this remains a critical component of patient care in the face of this season’s looming twindemic.
Chad Larson, NMD, DC, CCN, CSCS, holds a Doctor of Naturopathic Medicine degree from Southwest College of Naturopathic Medicine and a Doctor of Chiropractic degree from Southern California University of Health Sciences. He is a Certified Clinical Nutritionist and a Certified Strength and Conditioning Specialist with particular interest in advanced developments in the fields of endocrinology, orthopedics, sports medicine, and environmentally-induced chronic disease. Dr. Larson is an Advisor and Consultant on the Clinical Consulting Team for Cyrex Laboratories.
Mark Engelman, MD, is the Director of Clinical Consulting for Cyrex Laboratories. He is also the Founder and President of the Engelman Health Institute. His career history includes 23 years as the director of St. Joseph’s Medical Center emergency department; and a term as President of the Maricopa County American Heart Association. He is also the Founder and CEO of AmeriMed American Hospitals in Mexico; and is known as an expert speaker on emergency medicine both nationally and internationally.
A recent
study published in the journal Arthritis and Rheumatology, shows that
the prevalence of antinuclear antibodies (ANA)– the most common biomarker of
autoimmunity–has increased considerably in the United States in recent years.
Researcher
Gregg E. Dinse and colleagues at Social & Scientific Systems, Durham, NC, examined
the prevalence of ANA positivity in human subjects from three distinct time
periods between 1988 and 2012. In total, they had data from 14,211 individuals.
The findings were astounding. Based on their sample population, they estimated that:
· In
1988-1991, 11% of the US population, or 22 million individuals, were ANA-positive.
· In
1999-2004, this increased to 11.5%, or 27 million individuals.
· In
2011-2012, the number was 15.9%, or 41 million individuals.
The
authors note that prevalence of ANA increased in both genders over the last
30-plus years, but particularly in men. There were also marked increases in
adults aged 50 years or older of all racial and ethnic backgrounds, and in
non-Hispanic whites (Dinse GE, et
al. Arthr Rheumatol. 2020).
“These increases in ANA
prevalence were not explained by concurrent trends in weight
(obesity/overweight), smoking exposure, or alcohol consumption,” they write.
As a category, “Autoimmune Disease” includes over 100 debilitating conditions; it is no wonder so many people are affected. The article also emphasizes the need for clinicians to take a more comprehensive look at the individual, immune system “fingerprints” of patients with autoimmune conditions.
Immunophenotyping
The
immune system “fingerprint,” or “immunophenotype” as it is known in research
terms, reflects an individual’s immunologic makeup, and it has significant
implications in terms of how the immune system functions both in relation to
the body’s own tissues, as well as in response to exogenous pathogens.
Immunophenotyping
uses highly specific antibodies to identify various types of cells based on the
antigens and markers expressed on their surfaces, in their nuclei, or in their
cytoplasm. These techniques, based largely on flow cytometry, are widely used
in basic immunological research, as well as in cancer research and oncology
practice. They’ve enabled oncologists to identify and categorize certain types
of cancer, particularly leukemias, with great accuracy.
The immune system “fingerprint,” or “immunophenotype” as it is known in research terms...informs how each individual may react, or is reacting, to an environmental antigen, like a virus. In the context of the COVID-19 pandemic, this sort of information is essential to helping immunocompromised patients protect themselves.
Flow
cytometry utilizes light-scatter technology to detect and count specific cell types
present in a mixture of cells. It is preferred by top researchers because of
its quantitative accuracy and specificity.
Recently, however, interest in the technique has extended well beyond basic research labs and oncology centers.
That’s because these tests can give physicians much more detailed information about a patient’s immune system than we can obtain from standard Complete Blood Count (CBC) panels. We can gain unprecedented, in-depth views of our patients’ immune systems. This knowledge is critical to making informed clinical decisions.
Relevance for COVID Risk
Immune
system fingerprinting has relevance to the current COVID-19 pandemic.
We
know that patients with autoimmune diseases are at higher risk for COVID-19.
According to the Global
Autoimmune Institute, there are instances in which having an autoimmune
disease increases vulnerability to COVID-19 complications. In other cases,
contracting COVID-19 triggers pre-existing autoimmunity, leading to symptom
flares. Severe cases of COVID-19 have been associated with hyperactive immune
responses in chronically ill patients, as well as those who previously showed no
signs of autoimmunity.
A
pre-existing, but possibly undetected issue with the immune system may enable
the SARS-CoV-2 virus to move from the nose and throat, into the lungs, and to spread
to other parts of the body.
Immunocompromised
patients may not be able to manufacture the antibodies needed to prevent the
virus from entering cells. Likewise, individuals on immunosuppressive
medications such as corticosteroids are also at higher risk to be infected and
suffer more severe COVID-19 complications.
We live in an ever-changing world of complicated novel pathogens, such as COVID-19. While it is important that we research and understand each of them, we must also recognize that there is much more to the complex picture of an individual patient’s risks and outcomes.
Simplifying
a Complex Picture
As Hen-Avivi and Avraham
note in their 2018 paper, “There is, in fact, great heterogeneity in infection
outcome, from complete clearance of the pathogen to severe illness.
Understanding this variation remains elusive, despite its great potential to
equip us with new tools for the treatment of infectious diseases.”
A pre-existing, but possibly undetected issue with the immune system may enable the SARS-CoV-2 virus to move from the nose and throat, into the lungs, and to spread to other parts of the body
They propose that single-cell
analysis technologies and recent advances in single-cell RNA-seq technologies “allow
the detection of rare subpopulations that play important roles in host-pathogen
interactions.” These techniques can
provide “a ‘fingerprint’ of the immune cell types that are associated with the
ability of the host to clear a pathogen and, thereby, broaden our current understanding
of variation in susceptibility to infection within the population.” (Hen-Avivi S, Avraham R. Curr Opin Microbiol. 2018).
In
the clinic, immunophenotyping can give us a lot of information about the
integrity of a patient’s immune systems. It goes far beyond what we can obtain
from standard lab tests, which are not specific-enough or sufficiently detailed
to allow a thorough evaluation of a patient’s overall immune system health or the
risks of future diseases and complications.
Beyond
the CBC
For
example, unusually high or low white blood cell (WBC) counts obtained from a
complete blood count (CBC) may indicate that something is wrong, but they do
not usually reveal what is going on with the patient. Often, a CBC comes back
absolutely normal, but the patient could actually be suffering from immune
system dysfunction, immunodeficiency, hyper-inflammation, autoimmunity, allergies,
and hypersensitivities induced by environmental triggers.
Simply
stated, a stand-alone CBC panel is only one piece of the puzzle. Tests that
reveal various immunophenotypes can give us significantly more usable clinical
information.
Flow
cytometry actually separates and quantifies different types of cells by detecting
unique markers present on the cell surface. It is much more specific than
standard tests that attempt to quantify different immune cell types by
measuring cellular products such as cytokines and other signaling substances.
Since
lymphocytes make up 20-40% of an individual’s total white blood cells (WBCs),
understanding the lymphocyte sub-populations (like TH1, TH2, CD4, CD8, TH17,
Natural Killer Cells etc.) and their ratios is the foundation of a detailed
immune system fingerprint.
This
fingerprint informs how each individual may react, or is reacting, to an
environmental antigen, like a virus. In the context of the COVID-19 pandemic,
this sort of information is essential to helping immunocompromised patients
protect themselves.
Cyrex Laboratories’ a clinical laboratory specializing in functional immunology and autoimmunity, has recently developed a proprietary test panel called The Lymphocyte Map – Comprehensive Immunophenotyping of Lymphocytes, that provides comprehensive information on an individual’s unique immune system fingerprint. The Lymphocyte Map is the latest release in Cyrex’ innovative line of tests geared toward assessing “immune health.” In essence, it translates a host of complex flow cytometry data into an immune health analysis report.
Given
the wide prevalence of autoimmune conditions, and the ways that autoimmunity
heightens risk for infectious diseases, it makes good clinical sense to
consider running a Lymphocyte Map any time you would typically order a CBC. It
can provide indispensable information for guiding treatment decisions, and it
has the added benefit of helping practicing clinicians to better read and
comprehend the current medical literature at a time of unprecedented interest
in the immune system.
END
Chad Larson, NMD, DC, CCN,
CSCS, holds a Doctor of Naturopathic Medicine degree from Southwest College of
Naturopathic Medicine and a Doctor of Chiropractic degree from Southern
California University of Health Sciences. He is a Certified Clinical
Nutritionist and a Certified Strength and Conditioning Specialist with
particular interest in advanced developments in the fields of endocrinology,
orthopedics, sports medicine, and environmentally-induced chronic disease. Dr.
Larson is an Advisor and Consultant on the Clinical Consulting Team for Cyrex Laboratories.
Mark. Engelman, MD, is the
Director of Clinical Consulting for Cyrex Laboratories. He is also the Founder
and President of the Engelman Health Institute. His career history includes 23
years as the director of St. Joseph’s Medical Center emergency department; and
a term as President of the Maricopa County American Heart Association. He is
also the Founder and CEO of AmeriMed American Hospitals in Mexico; and is known
as an expert speaker on emergency medicine both nationally and internationally.