




Physicians and practice managers rejoice! For the first time in 30 years, the outpatient
Evaluation and Management codes (E/M) will undergo an historic overhaul by the American Medical Association (AMA) and Centers for Medicare and Medicaid Services (CMS). Many of the changes are for the better.
Any physician or coder who has felt frustrated when trying to tabulate the level of an E/M visit will feel relief at the new guidelines, which take effect January 1, 2021. The new E/M coding overhaul will decrease administrative burdens on doctors and practice managers.
The changes include updated requirements for documenting medical necessity and exams, elimination of “note bloat” by reducing redundancy in copying and pasting case notes, and consideration of the total time a physician spends on a patient.
“While these significant changes will require preparation and training, the overall benefits will be immense. The reduction of complicated coding structures and redundant paperwork will help reduce the hassle-factor, prevent physician burnout, and lead to better overall patient care.”
The Prolonged Visit codes have undergone a transformation as well, though those guidelines have not yet received final approval by CMS.
After extensive surveys of practitioners to determine what changes were needed, the AMA Workforce formed its Guiding Principles as follows:
1. To decrease administrative burden of documentation and coding.
2. To decrease the need for audits.
3. To decrease unnecessary documentation in medical records not needed
for patient care.
4. To ensure that payment for E/M is resource-based and has no direct goal for payment redistribution between specialties.
Times are Changing
Medical Necessity: Under the new guidelines, documentation for medical necessity of a home visit over an office visit will no longer be required. Also, the frustrating prohibition for same-day E/M by physicians of thesame group or specialty has been lifted. These changes will eliminate inconvenience for patients, who will no longer need to space appointments or delay medical care. It will also reduce the number of physiciansgoing unpaid for their exams.
Reduction of Redundant Documentation: No longer will physicians be required to copy and paste irrelevant notes fromprevious visits. This is a very good thing, because the requirements to e-enter outdated information unrelated to a chief complaint (CC)
led to “note bloat” and created a lot of additional work for auditors and coders. After January 1, 2021, physicians or Qualified Health Providers (QHP) may simply notate “the PHI has been reviewed and verified.”
Simplified Exams: The 1995 and 1997 Guidelines both include extensive Review of Systems (ROS)checklists. These requirements took a considerable amount of time, and were oftenirrelevant. The 2021 Guidelines now require only a medically relevant exam. For example, agynecologist will no longer be required to check eyes and ears.
Choose Your Coding Path: The 1995 and 1997 Guidelines had very complicated point systems for determining the coding levels for History, Physical Exam, and Medical Decision-Making. Time was only a factor if the time spent counseling or coordinating care for a patient was more than 50% of total face-to-face time with the patient or patient representative. Non-face to-face time such as consulting with other practitioners or reviewing charts, labs, and images were not considered at all.
“With the new 2021 Guidelines, physicians may now choose to code based on either the complexity of Medical Decision Making (MDM) or Total Time spent on that particular patient. This is the most significant change, and will truly enhance patient care.”
With the new 2021 Guidelines, physicians may now choose to code based on either the complexity of Medical Decision Making (MDM) or Total Time spent on that particular patient. This is the most significant change, and will truly enhance patient care.
“Total Time” encompasses the following:
• Preparing to see the patient (eg, review of tests)
• Obtaining and/or reviewing separately obtained history
• Performing a medically necessary and appropriate examination and evaluation
• Counseling and educating the patient/family/caregiver
• Ordering medications, tests, or procedures
• Referring and communicating with other health care professionals (when not reported separately)
• Documenting clinical information in the health record
• Independently interpreting results (not reported separately) and communicating results to the patient/family/caregiver
• Care coordination (not reported separately)
Prolonged Visit Codes: Many physicians are unaware of the Prolonged Visit Codes. Under previous guidelines allowed physicians to be paid for extended face-to-face time with the patient. But coding for this involved wrangling with very complicated time-tables
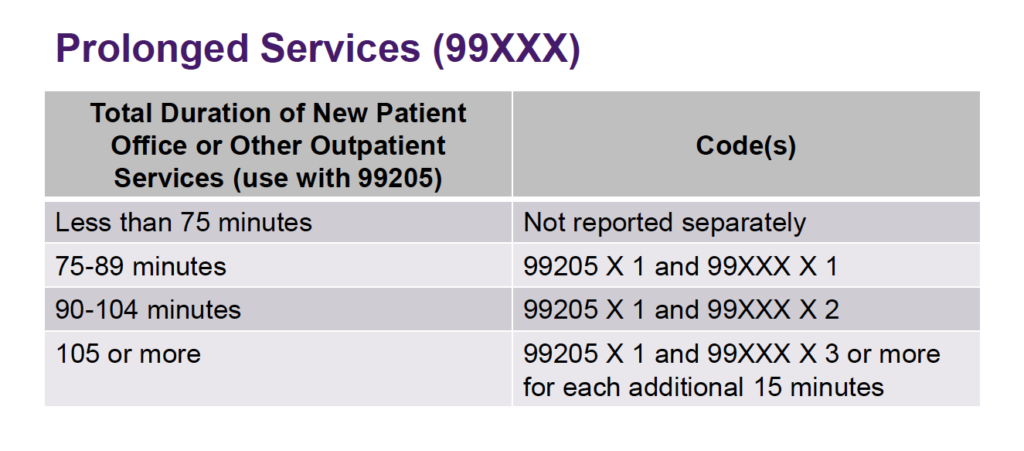
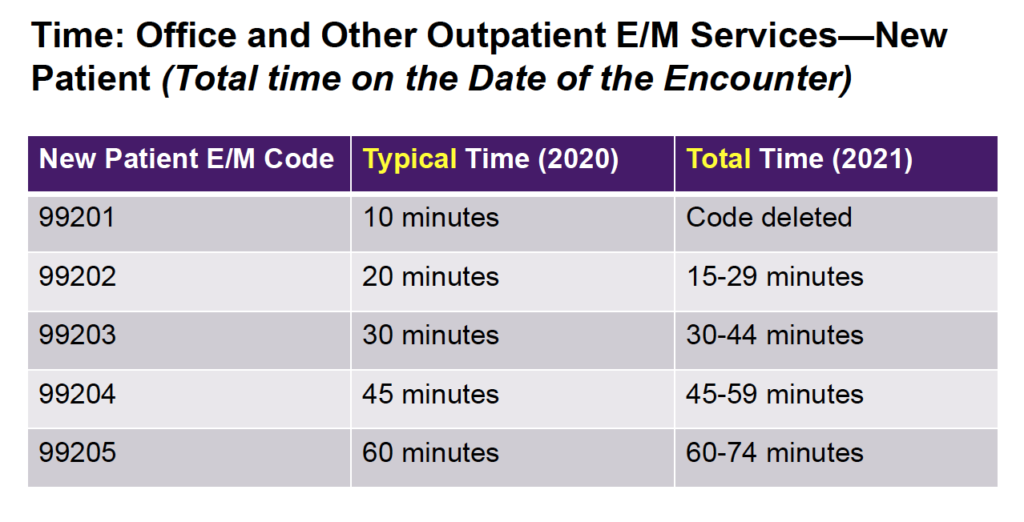
The new guidelines streamline the timetables for the primary E/M codes and prolonged codes. The E/M code levels increase by 10-minute intervals, and the prolonged codes are in increments of 15 minutes. See the improved timetables below.
I have spent thirteen years in medical administration and the last two working as a Corrective Exercise Specialist under both a Naturopathic Doctor and Medical Doctor. I know how onerous coding can be, and I believe these new guidelines will be a big improvement. I applaud the AMA and CMS for their openness and cooperation with practitioners across many different specialties.
While these significant changes will require preparation and training, the overall benefits will be immense. The reduction of complicated coding structures and redundant paperwork will help reduce the hassle-factor, prevent physician burnout, and lead to better overall patient care.
Likewise, the lowered need for audits will decrease administrative and financial burdens on the healthcare system.
Take advantage of the training tools the AMA offers at ama-assn.org to prepare yourself and your staff.
Stacy Collier is an independent practice management and billing consultant based in Anchorage, AK. She is also a certified personal trainer with a special focus in Corrective Exercise Therapy, helping people living with low back, shoulder, hip, and knee pain.
END


