



Traumatic Brain Injury (TBI) is usually related to a specific, unifying event in time, but it does not always have a unifying principle of diagnosis. There is an immense degree of variation in the ways TBI can present clinically. Likewise, there are a wide variety of therapeutic options helpful in managing the sequelae of TBI. Treatment needs to be guided by the presentation.
always have a unifying principle of diagnosis. There is an immense degree of variation in the ways TBI can present clinically. Likewise, there are a wide variety of therapeutic options helpful in managing the sequelae of TBI. Treatment needs to be guided by the presentation.
In the last edition of Holistic Primary Care, we explored how to recognize a TBI, an important issue given the rising incidence of these injuries (read Traumatic Brain Injuries are Increasingly Common, But Easily Missed, from our Summer 2010 edition). A recent article in the New York Times about Mets’ outfielder Jason Bay’s concussion underscored the need to evaluate injured athletes for TBI, and the growing number of veterans returning from Iraq and Afghanistan with head trauma is making TBI a top-line clinical issue these days.
This article focuses on treatment options, and how to apply them. Many treatments for head trauma are well researched and have been used in holistic medicine for years. Diet, targeted supplementation, and homeopathic remedies are all highly effective for patients with head injuries. One treatment that is very well researched but generally under-utilized is neurofeedback, a form of biofeedback guided by electroencephalography. By combining modalities you can optimize outcomes and greatly improve patients’ quality of life.
Vitamin D, Magnesium & Calorie Restriction
Tailored supplementation is an extremely important part of treating TBI, and vitamin D is one of the key nutrients to consider. Earlier this year, Jessica Schneiders from Rijnstate Hospital in Arnhem, Netherlands, presented data at the European Congress of Endocrinology, showing that vitamin D stores are depleted after a TBI. The resulting vitamin D deficiency is associated with post-TBI chronic fatigue, a common complaint among TBI patients.
Vitamin D is vital for people who’ve had brain injuries, regardless of their symptoms. Available data support doses in the range of 3,000-5,000 IU per day, for a minimum of three months (Cekic M, et al. Front Neuroendocrinol. 2009; 30(2): 158-72). It makes sense to retest after three months, to see if serum levels have increased. However, be aware that prolonged exposure to high levels of Vitamin D may increase the risk of kidney stone formation. (For more information about health risks of excess vitamin D, visit http://ods.od.nih.gov/factsheets/vitamind.asp#h8).
Along with vitamin D, magnesium is also helpful following neurological injury. This observation was published nearly 20 years ago! (McIntosh TK, et al. Brain Res.1989; 482(2): 252-60). Magnesium and vitamin D seem to be synergistic, each improving the absorption and physiological function of the other (http://www.vitamindcouncil.org/). Magnesium is a co-factor for vitamin D metabolism. In fact, if you have a patient who is supplementing with vitamin D for any clinical condition, but not showing improvement, think about magnesium deficiency!
Acute brain injury can lead to secondary injuries after the initial damage. Some researchers believe this is related to a loss of magnesium post-TBI. (van den Heuvel C, Vink R. Clin Calcium. 2004;14(8): 9-14; Werner C, Engelhard K. Br J Anaesth. 2007; 99(1): 4-9).
Two recent papers support the notion that magnesium deficiency leads to hyper-excitability of the nervous system (Nielsen FH. Nutr Rev. 2010;68 (6):333-40; Barbagallo M, Dominguez LJ. Curr Pharm Des. 2010; 16(7): 832-9). This may be the reason that anxiety, insomnia, spasticity, and other symptoms of hyper-excitability are common in TBI patients. In practice, magnesium supplementation can be extremely effective, at dose levels of 125 mg/day.
Essential fatty acids (EFAs) also have a role post-TBI. They play a role in the neuronal healing process, as has been elucidated in several recent studies (Chang CY, et al. Acta Neurol Taiwan. 2009;18(4):231-4; Logan AC. J Neurotrauma. 2008 Dec;25(12):1499; Wu A, et al. J Neurotrauma. 2007; 24(10): 1587-95). Three grams of omega-3 fatty acids daily, for 90 days, reduces inflammation and protects the nervous system.
Nutritional supplementation for the care of TBI should not be done in isolation; dietary changes are also important. Calorie restriction and ketogenic diets are highly beneficial (Kossoff EH, Rho JM. Neurotherapeutics. 2009; 6(2): 406-14). When combined with exercise, calorie restriction has been shown to rejuvenate the synapses of brain injured mice. The reasons for these benefits are not completely understood but calorie restriction and ketogenic diets may improve mitochondrial function while reducing inflammation throughout the body. Ketone bodies formed as a result of a ketogenic diet may protect neurons from various injuries (Maaouf M, et al. Brain Res Rev. 2009; 59(2): 293-31).
Other lines of research indicate that gluten elimination may help some patients following TBI (Abenavoli L. J Am Diet Assoc. 2008;108 (12):1995; Tursi A, et al. Dig Dis Sci. 2006;51(10):1869-74.). Given the strong connection between the gut and the brain, it is important to recognize that TBI can often result in digestive problems. Think about gluten elimination in any TBI patient who has digestive difficulties.
Homeopathy After Head Injury
Homeopathy can be extremely helpful in the treatment of patients following TBI. Ideally, patients should undergo a thorough homeopathic work up by a well-trained practitioner, as each case is unique. That said, I’ve found three remedies to be effective for many patients. They are Arnica Montana, Aconite and Natrum Sulphuricum.
Arnica is useful in cases where the injury results in slipping into and out of consciousness, or the patient often experiences “being in a fog.” These patients may act as if nothing is wrong, or try to minimize the seriousness of the incident, but they may show or report bluish bruising immediately after injury.
Aconite can be helpful following near-death injuries that leave the person living in a perpetual state of shock. Natrum Sulphuricum is effective for those who are depressed or suicidal, both of which are fairly common states following TBI. These patients may manifest a grief component as well. These patients may be using street drugs or excessive sexual activity to compensate for their grief or to mask their depression. Military veterans with TBIs have benefited from treatment with Natrum Sulphuricum on many occasions.
Neurofeedback: Non-invasive, Highly Effective
One of the most exciting therapies for TBI is neurofeedback, also known as neurotherapy, or EEG-biofeedback. Essentially, it is a form of biofeedback guided by electroencephalography.
There are a number of different neurofeedback systems and protocols, but generally speaking they all involve connecting the patient to a computer-based system via electrodes with at least three different points of contact to the scalp and ears. The process begins by using EEG to create a map of the patient’s brain, and to identify the particular point or points in the brain that may not be functioning optimally.
Depending upon the type of neurofeedback, the patient may sit in the chair from seconds to up to an hour. The system monitors brain waves, and may also send impulses back into the brain, though they are at such a low level that the person generally does not feel it. A patient’s experience will vary, based on the type of system being used. Traditional neurofeedback is similar to playing a computer game only the player influences the action of the game with his or her brainwaves rather than via a hand-held controller.
There are literally hundreds of neurofeedback systems now available, ranging in cost from $500 to $20,000. Each manufacturer has its own training requirements and some are more diligent about those requirements than others.
Most of my experience in treating TBI is with the Low Energy Neurofeedback System (LENS). LENS requires 40% fewer sessions than traditional neurofeedback; patients are generally seen weekly for about 10-20 weeks including the mapping. LENS also uses a much lower wattage than traditional neurofeedback (almost 1,000,000 times fewer watts per centimeter squared (W/cm2). With LENS, each point is treated for just seconds.
Neurofeedback is based on a new understanding of what actually happens to neurons following trauma. Physicians and neuroscientists used to believe that injured, non-functioning neurons are “dead.” But we have since learned that they are, in fact, dormant and can be reawakened. LENS appears to awaken injured neurons, ultimately resulting in better cognitive and behavioral function, and reduced symptom burdens. LENS is not a method for entrainment, but rather a method for accurately sending minute electrical signals into the brain to allow for the neurons to change their response. (For more information about LENS please visit www.ochslabs.com).
Generally, I start by mapping a patient’s brain, measuring frequency and amplitude at 21 distinct points. Once the map is complete, we analyze it to determine the course of treatment. The map is based on two core aspects of brain waves: amplitude and frequency. Brainwaves are grouped into several distinct categories based on their wavelength (the inverse of frequency): delta, theta, alpha, low beta, mid-beta, high beta and gamma. Essentially what we are mapping is the dominant brainwave frequencies in the brain, which tell us a lot about how specific brain regions are functioning. Table 1 outlines, in general terms, what each type of brain wave might reflect.
Delta Dominance
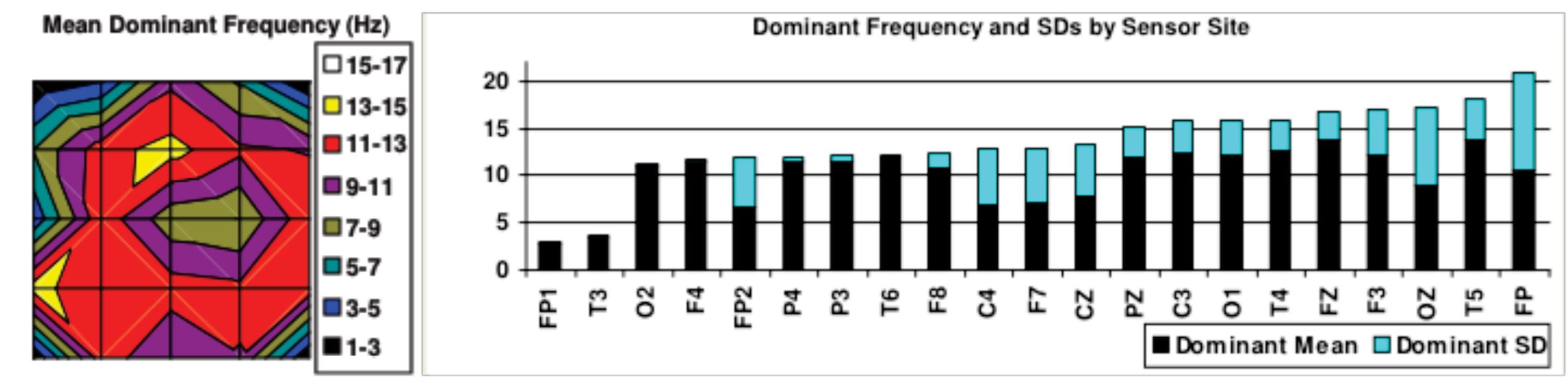
In post-TBI patients, delta waves tend to be dominant. Delta waves are characteristic of sleep, suggesting that the brain is inappropriately “asleep” during waking hours (Figures 1 & 2). This is one of the reasons why insomnia is so common among people with TBI. According to Kayle Sandberg-Lewis, ND, a naturopathic physician with extensive experience treating TBI, the injured brain already believes itself to be asleep so it doesn’t allow the body to go to sleep. Insomnia is often the first thing that improves in TBI patients who receive neurofeedback.
Brainwave amplitudes may also be anomalous in people with head injuries. High-amplitude waves regardless of frequency are associated with a brain that is working too hard; very low amplitude waves indicate brain regions that are not working enough. A pattern of higher amplitudes correlates clinically with complaints of anxiety and hyperexcitability. In my experience, TBI patients who present with a lot of anxiety often show excessively high amplitudes that normalize following treatment.
Brainwave patterns can vary considerably from patient to patient, but generally speaking, the EEG maps of people who have had TBIs show two distinct features: a predominance of high amplitude delta waves not generally seen in a healthy brain, and abnormally flattened or elevated amplitudes in other non-delta waves. However, some TBI patients show high delta amplitudes without a corresponding dominance of delta frequency.
Figure 1: Shows highly elevated delta amplitudes. This was from a patient with multiple head injuries over the course of twenty years.
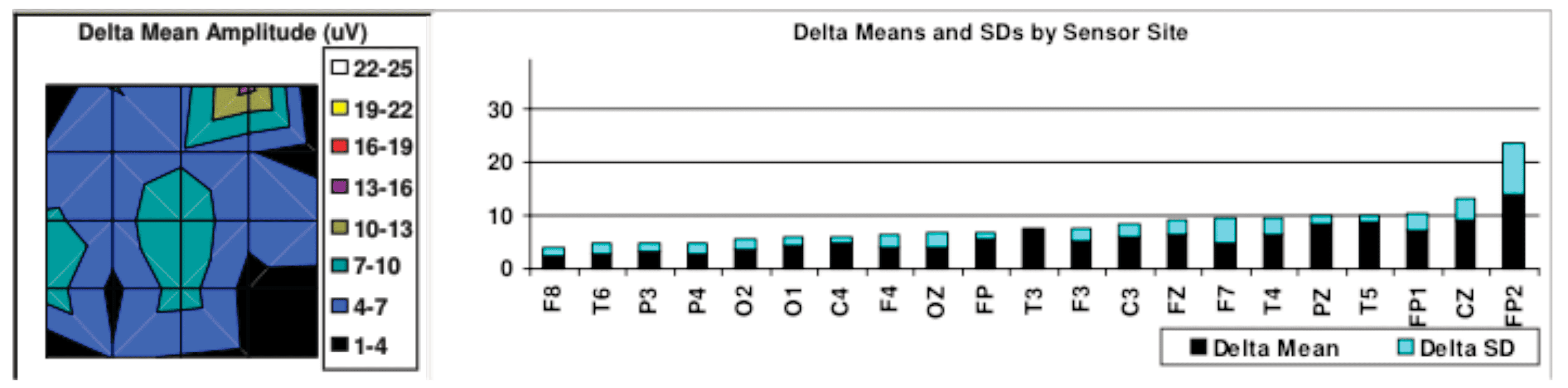
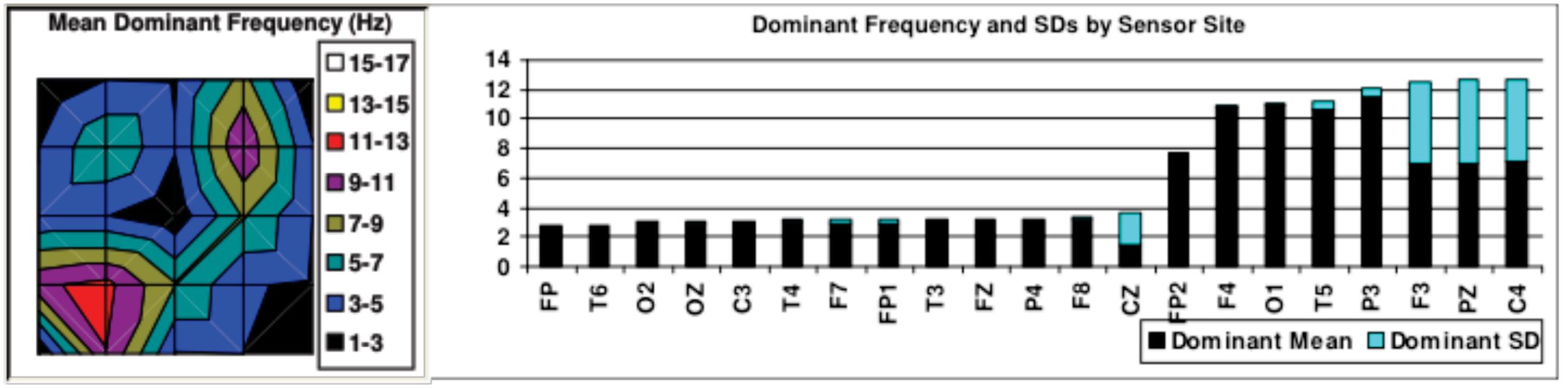
Figure 2: Dominant Frequencies showing that most of this patient’s brain is in delta waves even when awake.
“Awakening” Neurons, Improving Function
Recent studies indicate that neurofeedback has an 80% efficacy in treating the sequelae of TBI. Reported improvements include: reduced anxiety, improved memory, attenuation of cognitive disturbances, elimination of behavior problems, improved organizational and executive function, better attention, reduced pain, dissociation, and mood disturbances (Hammond DC. J Neurotherapy. 2003, 7(2): 25-52. Bounias M, et al. J Neurotherapy. 2002: 6(1) 23-38.2002).
While we know the efficacy, we do not understand the mechanism. Functional changes in the brain do occur in response to neurofeedback (Lévesque J, et al. Neurosci Lett. 2006.394(3): 216-21) but the exact mechanism is not understood. Many theories have been postulated. For a thorough review of LENS neurofeedback, I highly recommend the book, The Healing Power of Neurofeedback, by H. Stephen Larsen, PhD. Dr. Larsen worked closely with Len Ochs, PhD, who pioneered the technique.
Since I began practicing neurofeedback, I have worked with patients who’ve had car accidents, military veterans, victims of domestic violence and injured athletes. No two cases are the same, and the uniqueness of each presentation makes this type of work both challenging and extremely interesting!
One case involved a 60-year-old female who had had multiple injuries, including a car accident during her first pregnancy, many years prior. She was unable to get pregnant the second time without Clomid, possibly due to the accident. When I saw her, she presented with fatigue, insomnia, memory loss, weight gain, constipation and a variety of other symptoms.
We began a program of weekly neurofeedback sessions, augmented by supplementation with Vitamin D (5,000 IU/day), magnesium (125 mg/day), and homeopathic pituitary gland 4 CH (10 drops, twice daily). Sleep improved almost immediately, as did fatigue and constipation. She lost weight and, after about 12 weeks, her memory greatly improved as well.
Figs. 3 and 4 show this patient’s dominant frequencies at baseline and after completion of treatment. Her brain went from mostly slow wave activity (delta and theta waves) before treatment, to higher frequency activity, which is more characteristic of an alert adult brain. Not only had her sleep improved, her entire sleep/wake rhythm had shifted from one of sleeping at 1 AM and waking at 6 AM, to one of sleeping at 10 PM and awakening at 6 or 7 AM. She was not only getting more sleep but getting a better quality sleep.
Figure 3: Before treatment, the frequency map shows much of the patient’s brain in delta and theta brainwave activity, which is inappropriate for the waking state.
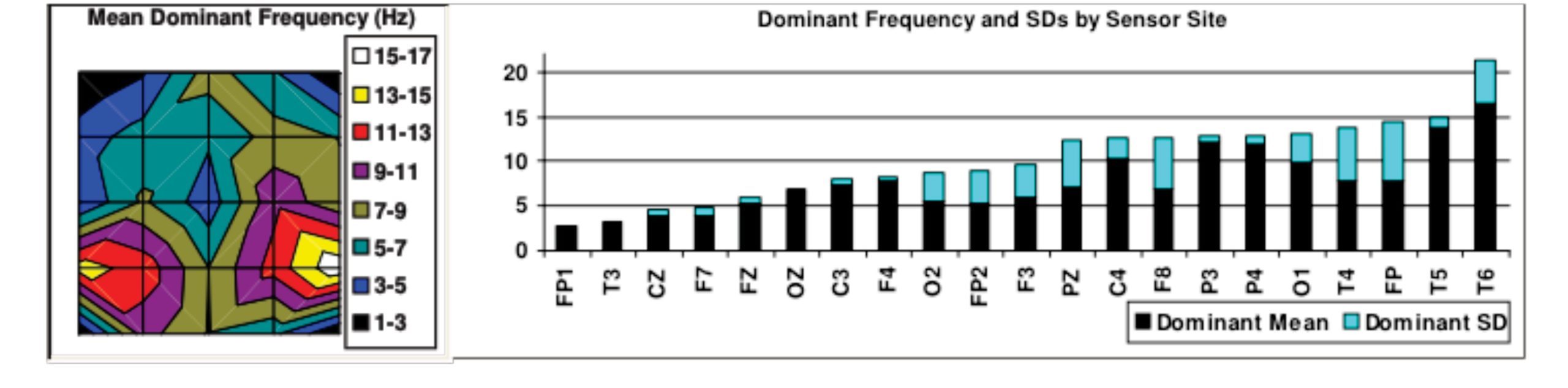
Figure 4: Following neurofeedback, there are still some residual delta points, but the majority of brain regions are in alpha and low-beta activity, appropriate for an adult brain in an alert state.
Images courtesy of Dr. Gil Winkelman
We are just beginning to learn how brain injury affects the body and why it causes such disparate symptoms in different patients. Generally a combination of approaches is the most effective way to work. In my practice, I combine neurofeedback with targeted supplementation, and specific treatments for the organ systems most affected by the injury. This provides symptomatic relief while simultaneously treating the deeper pathology.
One of the most important things to remember is that TBIs can manifest in many ways, not all of which will immediately register to you as “neurologic.” So if you have a patient with a chronic condition that is not responding to treatments that generally work, think about the possibility of TBI, and make sure to ask patients about possible incidents of head injury.
Gil Winkelman ND, MA is a Naturopathic Physician with over 15 years experience treating people with traumatic brain injury. He has worked with many people with TBI and other ailments. He is also the founder of iCaduceus: The Clinician’s Alternative, a database pairing Western diagnoses with non-pharmacological treatments for over 400 conditions. He practices in Portland, OR with his wife Christie Winkelman, ND, MA.


